Table of Contents
Overview – Valvular Heart Disease
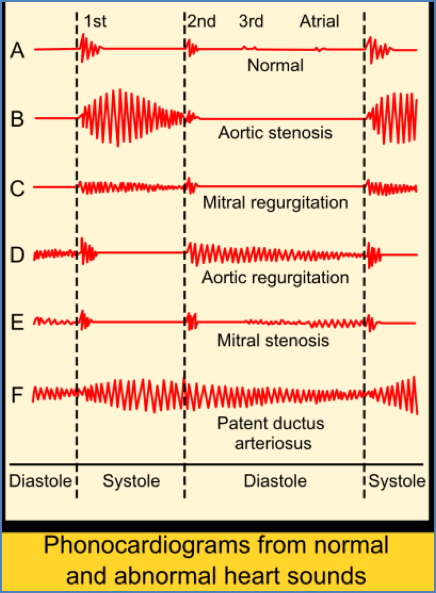
Valvular heart disease refers to damage or dysfunction of one or more of the heart valves, leading to stenosis (narrowing) or regurgitation (leakage). The most commonly affected valves are the mitral and aortic valves, often resulting from rheumatic fever, degenerative changes, or congenital defects. Accurate identification of murmurs and underlying pathology is essential for diagnosis, management, and prevention of complications such as heart failure and arrhythmias.
Aetiology
Common Valve Lesions and Causes:
| Valve Lesion | Common Causes |
|---|---|
| Mitral Stenosis | Rheumatic Fever (Post-inflammatory scarring) |
| Mitral Regurgitation | Mitral Valve Prolapse (Myxomatous degeneration), Rheumatic Fever, MI (papillary muscle dysfunction), Infective Endocarditis, Chordae rupture, Dilated cardiomyopathy, Congenital defects |
| Aortic Stenosis | Age-related calcification, Rheumatic Fever |
| Aortic Regurgitation | Aortic root dilation (age, hypertension), Rheumatic Fever, Infective Endocarditis, Marfan’s Syndrome, Syphilitic Aortitis, Rheumatoid Arthritis, Ankylosing Spondylitis |
Less Common Valvular Lesions:
| Lesion | Cause/Association | Murmur Timing |
|---|---|---|
| Pulmonary Stenosis | Congenital, Rheumatic | Systolic |
| Pulmonary Regurgitation | Pulmonary Hypertension | Diastolic |
| Tricuspid Stenosis | Rheumatic | Diastolic |
| Tricuspid Regurgitation | RV Dilation (e.g., infarction) | Systolic |
Mitral Stenosis
Aetiology
- >99% due to Rheumatic Heart Disease
Pathophysiology
- Recurrent episodes of acute rheumatic fever trigger an autoimmune response → fibrosis of the mitral valve → progressive narrowing (stenosis) of the orifice.
Clinical Features
Symptoms:
- Congestive cardiac failure (CCF):
- Exertional dyspnoea
- Orthopnoea
- Paroxysmal nocturnal dyspnoea (PND)
- Wet cough due to pulmonary oedema
Signs:
- Low-volume pulse
- Mid-diastolic rumbling murmur, loudest at the apex, during expiration, radiating to the axilla
- “Mitral facies” – malar (butterfly) rash over cheeks and nose
- Pulmonary hypertension and RV failure signs:
- Right ventricular heave
- ↑ JVP
- Pulsatile liver
- Ascites
- Peripheral oedema
Investigations
- ECHO: Diagnostic modality of choice (confirms valve morphology and gradient)
- ECG: May show atrial fibrillation, left atrial hypertrophy (LAH), and right ventricular hypertrophy (RVH)
- CXR: LA enlargement, pulmonary congestion
Management
Medical:
- Manage atrial fibrillation (rate/rhythm control, anticoagulation with warfarin)
- Triple therapy for CCF: ACE inhibitor + β-blocker + diuretic
Surgical:
- Mitral valvuloplasty (balloon repair) if anatomy allows
- Mitral valve replacement for severe or calcified disease


Mitral Regurgitation
Aetiology
- Myxomatous degeneration (mitral valve prolapse)
- Rheumatic fever
- Infective endocarditis
- Ischaemic heart disease (e.g. papillary muscle rupture post-MI)
Pathophysiology
- Myxomatous degeneration: weakening of connective tissue → prolapse and regurgitation
- Infective endocarditis: valve edge vegetations prevent closure
- Ischaemia: papillary muscle dysfunction → failure of systolic coaptation
Clinical Features
Symptoms:
- Exertional dyspnoea
- Wet cough (pulmonary oedema)
Signs:
- High-pitched pansystolic murmur, best heard at the apex, radiates to the axilla, louder during expiration
- Left parasternal heave (due to LA enlargement)
Investigations
- ECHO: Diagnostic (confirms regurgitant volume, leaflet mobility)
- ECG: LAH, left ventricular hypertrophy (LVH)
- CXR: Cardiomegaly (LA and LV), pulmonary venous congestion
Management
Medical:
- CCF triple therapy: ACE inhibitor + β-blocker + diuretic
Surgical:
- Mitral valve repair (valvuloplasty) preferred when feasible
- Mitral valve replacement for advanced or unrepairable pathology


Aortic Stenosis
Aetiology
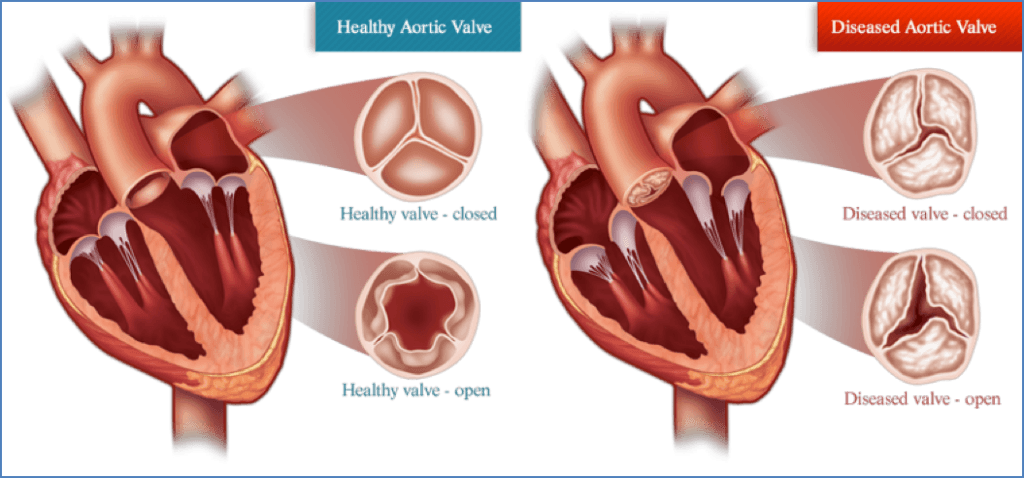
- Age-related calcification (most common; degenerative “wear & tear”)
- Rheumatic heart disease (accounts for ~10% of cases)
Pathophysiology
- Progressive fibrosis and calcification of the aortic valve → reduced leaflet mobility → narrowed outflow tract
- Leads to increased left ventricular pressure → hypertrophy and eventual failure
Clinical Features
Symptoms – “Aortic Stenosis Triad”:
- Angina – from increased oxygen demand due to LV hypertrophy
- Exertional dyspnoea – from congestive heart failure
- Syncope/dizziness – due to reduced cerebral perfusion on exertion
Signs:
- Displaced apex beat (LV hypertrophy)
- Loud ejection systolic murmur, best heard at the 2nd right intercostal space, radiates to carotids
- Louder on expiration
- ± Ejection click or systolic thrill
- Signs of CCF: pulmonary oedema, dyspnoea
Investigations
- ECHO: Diagnostic gold standard (confirms stenosis severity and valve structure)
- ECG: Left ventricular hypertrophy (LVH), strain pattern
- CXR: May show valve calcification, cardiomegaly, pulmonary venous congestion
Management
- Symptomatic disease requires intervention:
- Aortic valve replacement is the definitive treatment
- Balloon valvuloplasty is an option in select patients (e.g. non-surgical candidates)

Aortic Regurgitation (Aortic Incompetence)
Aetiology
- Aortic root dilation due to:
- Age or hypertension
- Syphilitic aortitis
- Connective tissue disorders (e.g. Marfan’s syndrome)
- Others: Rheumatic heart disease, infective endocarditis, ankylosing spondylitis
Pathophysiology
- Dilation of aortic root → poor leaflet coaptation → regurgitation during diastole
- Leads to volume overload in LV → eccentric hypertrophy → heart failure
Clinical Features
Symptoms – “Aortic Triad”:
- Angina – increased LV oxygen demand
- Exertional dyspnoea – early symptom of heart failure
- Syncope/dizziness – due to ↓CO and hypotension
Signs:
- Waterhammer pulse – bounding and rapidly collapsing
- Displaced apex beat (LV enlargement)
- Early diastolic decrescendo murmur, best heard at right 2nd intercostal space, louder on expiration
- Tachycardia – compensatory mechanism
Investigations
- ECHO: Diagnostic (quantifies regurgitant volume and LV function)
- ECG: Left atrial and ventricular hypertrophy (LAH, LVH)
- CXR: Cardiomegaly, pulmonary oedema
Management
Medical:
- Vasodilators (reduce afterload)
- Congestive heart failure therapy: ACE inhibitors + β-blockers + diuretics
Surgical:
- Aortic valve replacement when symptomatic or in severe AR with LV dysfunction


Tricuspid Valve Disease
Aetiology
Tricuspid Stenosis:
- Rheumatic fever (most common acquired cause)
- Congenital
- Carcinoid syndrome
- Endomyocardial fibroelastosis
Tricuspid Regurgitation:
- Right ventricular (RV) dilation – most common cause
- Infective endocarditis
- Rheumatic fever
- Congenital: Ebstein anomaly, atrioventricular (AV) cushion defects
- Carcinoid syndrome
- Tricuspid prolapse, trauma
Symptoms
- Features of right heart failure:
- Fatigue
- Pedal oedema
- Abdominal pain (liver congestion)
- Ascites
- Dyspnoea (especially if right-sided forward failure)
Signs
Pulse:
- Irregularly irregular if atrial fibrillation present
- Low-volume pulse
JVP findings:
- Prominent ‘a’ waves in tricuspid stenosis
- Large ‘v’ waves in tricuspid regurgitation
- Raised JVP
- Kussmaul’s sign (rise in JVP with inspiration)
Precordial findings:
- Left parasternal heave (in tricuspid regurgitation)
- Tricuspid stenosis: Diastolic murmur at 4th left intercostal space
- Tricuspid regurgitation:Holosystolic murmur at left lower sternal border, may have an ejection component
- All right-sided murmurs typically louder on inspiration, except pulmonary ejection click
Investigations
- ECG:
- Tricuspid stenosis: Right atrial enlargement
- Tricuspid regurgitation: RA enlargement, RV hypertrophy, atrial fibrillation
- CXR:
- Stenosis: Right atrial dilation without pulmonary artery enlargement
- Regurgitation: RA and RV enlargement
- Echocardiography:
- Gold standard for assessing structure and function
Management
- Supportive care:
- Surgery:
- Valve intervention typically dictated by concurrent need for left-sided valve or congenital repair
Pulmonary Valve Disease
Aetiology
Pulmonary Stenosis:
- Usually congenital
- Rare causes: Rheumatic, carcinoid syndrome
Pulmonary Regurgitation:
- Secondary to valve ring dilatation, often due to:
- Pulmonary hypertension (secondary to mitral stenosis, COPD, recurrent pulmonary emboli)
- Rheumatic disease
- Infective endocarditis
Symptoms
- Chest pain
- Syncope
- Dyspnoea
- Leg oedema (from RV failure and congestive heart failure)
Signs
Pulmonary Stenosis:
- Systolic murmur at 2nd left intercostal space
- May hear a pulmonary ejection click
- Variable intensity of P2, and right-sided S4
Pulmonary Regurgitation:
- Early diastolic murmur at the base
- Graham Steel murmur: Diastolic murmur at 2nd–3rd left ICS, louder on inspiration
Investigations
- ECG: Right ventricular hypertrophy
- CXR:
- Enlarged pulmonary arteries if pulmonary hypertension
- Enlarged right ventricle
- Echocardiography + Doppler: Diagnostic – assess valve morphology and flow gradients
Management
- Infective endocarditis prophylaxis
- Pulmonary regurgitation:
- Often well tolerated
- Valve replacement only if severe
- Pulmonary stenosis:
- Balloon valvuloplasty depending on severity
Summary – Valvular Heart Disease
Valvular heart disease encompasses a range of conditions affecting the heart valves, leading to stenosis or regurgitation. Common causes include rheumatic fever, age-related degeneration, infective endocarditis, and connective tissue disorders. Accurate auscultation, imaging, and timely intervention are critical to preventing heart failure, arrhythmias, and reduced quality of life. For broader context, see our Cardiovascular Overview page.