Table of Contents
Overview – Arrhythmias
Arrhythmias are abnormal rhythms of the heart caused by disrupted electrical conduction. This guide reviews key ECG findings, core mechanisms like re-entry and after-depolarisations, and the classification and management of common tachycardias, bradycardias, and conduction blocks. You’ll also learn how to recognise life-threatening patterns like ventricular fibrillation or complete heart block, and the pharmacological or interventional strategies used to manage them.
Characteristics of a Normal ECG
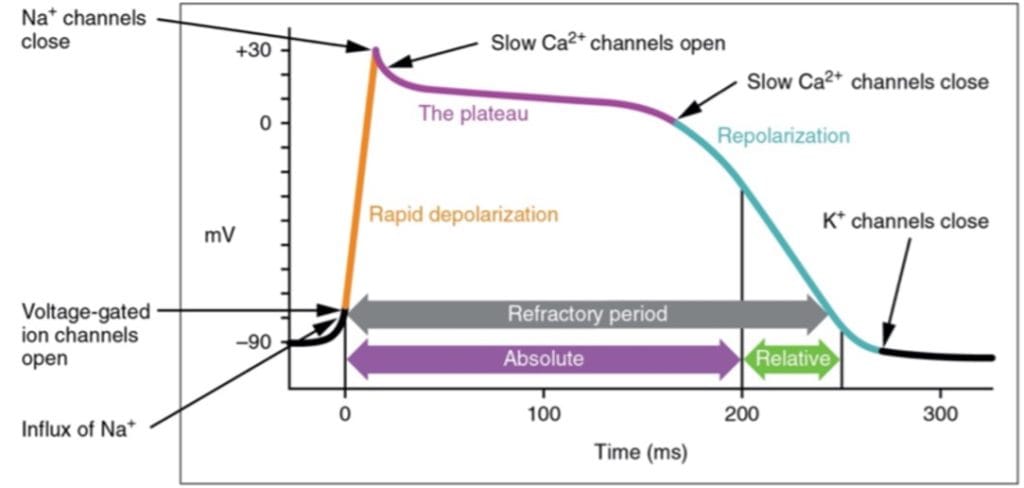
A baseline understanding of normal cardiac electrophysiology is essential for recognising arrhythmias.
- Sinus Rhythm/Rate:
- 60–100 bpm
- Originates from the sinoatrial (SA) node
- Intrinsic rate is higher, but suppressed by parasympathetic tone
- P-Wave:
- Rounded
- 0.5–2.5 mm tall
- Duration <0.1 seconds
- PR Interval:
- Fixed
- Duration: 0.12–0.20 seconds
- QRS Complex:
- Clean, sharp
- Amplitude <25 mm
- Duration: 0.06–0.12 seconds
- QT Interval:
- 0.35–0.45 seconds
- ST Segment:
- ≈0.08 seconds duration
- T-Wave:
- Prominent, rounded
- <5 mm (limb leads), <10 mm (precordial leads)
- Duration: 0.1–0.25 seconds
- U-Wave:
- Small (0.5 mm) deflection after T-wave
- Same polarity as T-wave
- Best seen in V2–V3

Mechanisms of Tachyarrhythmias
1. Re-entry (Re-entrant Tachycardia)
- Most common mechanism (≈75% of tachycardias)
- Involves an “ectopic focus” acting as a rogue pacemaker
- Common causes:
- Ischaemic heart disease
- Electrolyte disturbances
- Ion channel mutations
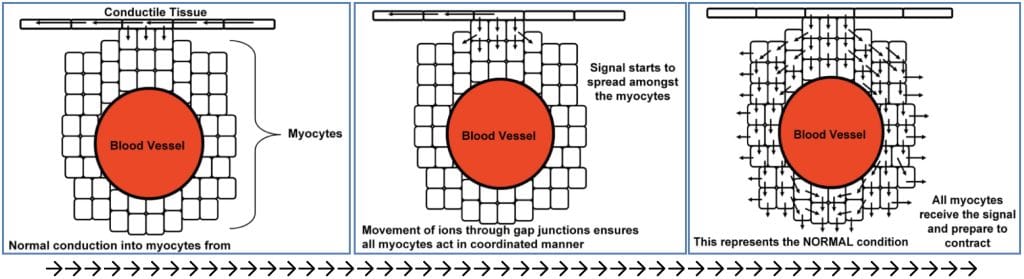
- Pathophysiology:
- Normally, an impulse travels through conductile and then contractile tissue.
- If a transient block occurs, re-entry can develop as the impulse loops back through previously depolarised tissue.
- Can produce isolated ectopic beats or sustained tachyarrhythmias.

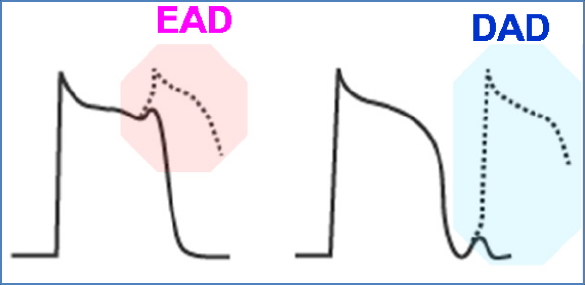
2. Early After-Depolarisations (EADs)
- Occur during the repolarisation phase (Phase 2 or 3)
- Triggered by increased action potential duration
- Mechanism:
- As the plateau phase prolongs, sodium channels may re-activate during their relative refractory period
- This premature depolarisation can initiate abnormal beats
- Associated arrhythmias:
- Torsades de Pointes
- Polymorphic ventricular tachycardia
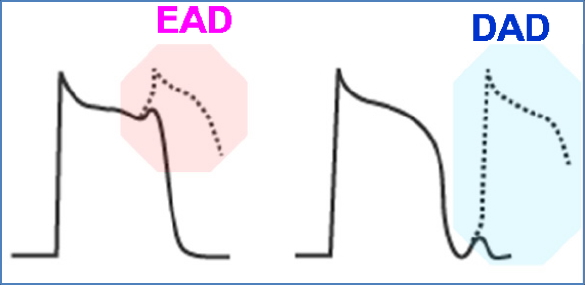
3. Delayed After-Depolarisations (DADs)
- Occur after full repolarisation (Phase 4)
- Triggered by intracellular calcium overload
- Most commonly linked to Digoxin toxicity
- Mechanism of Digoxin:
- Inhibits Na⁺/K⁺ ATPase → ↑intracellular Na⁺
- This disrupts the Na⁺/Ca²⁺ exchanger → ↑intracellular Ca²⁺
- More positive resting membrane potential → increased excitability
- Results in:
- Premature or multiple action potentials
- Tachyarrhythmias
Digoxin & Delayed After-Depolarisations

Supraventricular Tachycardias
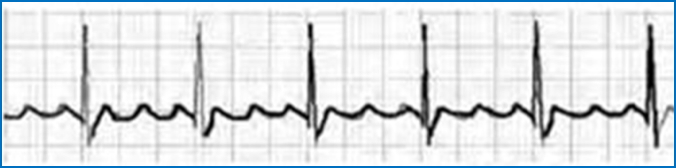
Sinus Tachycardia
- Defined as sinus rhythm >100 bpm
- ECG: Shortened T-P interval, all waves visible
- Physiological causes: Exercise, caffeine, sympathetic stimulation
- Pathological causes: Fever, hypovolaemia, pulmonary embolism
- Management:
- Carotid sinus massage
- β-blockers if symptomatic

Atrial Premature Beats (APBs)
- Single ectopic P-wave → ectopic QRS
- Often asymptomatic
- Management:
- Usually none
- β-blocker or calcium channel blocker if symptomatic

Atrial Flutter
- Atrial rate ≈ 300 bpm
- ‘Sawtooth’ P-waves
- Variable AV conduction (e.g., 2:1, 4:1)
- Mechanism: Re-entry circuit
- Common in: Pre-existing cardiac disease
- Management:
- Rate control: β-blockers, calcium channel blockers (Verapamil), digoxin
- Rhythm control: Electrical cardioversion
- Catheter ablation
Atrial Fibrillation (AF)
- Atrial rate ≈ 350–600 bpm, irregular QRS rhythm
- No distinct P-waves
- Causes (mnemonic “PIRATE SHIV”): PE, IHD, rheumatic heart disease, anaemia, thyrotoxicosis, alcohol, sepsis, HTN, iatrogenic, valvular disease
- Complications:
- Hypotension (↓CO)
- Pulmonary congestion
- Thromboembolism (stroke risk)
- Management:
- Rate control: β-blockers, Verapamil, digoxin
- Anticoagulation: Warfarin or DOACs
- Cardioversion: Medical (e.g. amiodarone) or electrical

Paroxysmal Supraventricular Tachycardia (PSVT)
- Sudden onset, regular tachycardia (>130 bpm)
- Usually due to atrial re-entry
- Diagnosis:
- ECG
- Adenosine challenge (slows SA node; diagnostic if rate slows)
- Management:
- Rate control (as above)
- Definitive: Catheter ablation

Ventricular Tachycardias
Premature Ventricular Complexes (PVCs)
- Additional, wide QRS complexes without preceding P-waves
- Isolated PVCs often benign, especially in healthy young adults
- Causes:
- Heart disease
- Hypokalaemia
- Hypoxia
- Management:
- Often none
- Potassium correction
- β-blocker if symptomatic

Ventricular Tachycardia (VT)
- ≥3 consecutive PVCs
- Sustained if >30 seconds
- Wide QRS, absent or unclear P- and T-waves
- Mechanism: Re-entry
- Management:
- Cardioversion
- Antiarrhythmics (e.g. Procainamide)

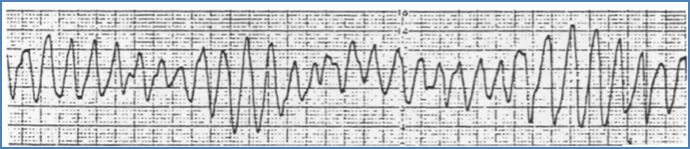
Ventricular Fibrillation (VF)
- Chaotic, disordered depolarisation
- No cardiac output → cardiac arrest
- Commonly follows PVCs or VT
- Management:
- Immediate defibrillation
- CPR
- Antiarrhythmics

Torsades de Pointes
- Polymorphic VT with changing QRS amplitude
- ECG shows ‘twisting’ pattern
- Causes:
- Long QT syndrome
- Drugs (K⁺ channel blockers)
- Electrolyte abnormalities (hypokalaemia, hypomagnesaemia)
- Management:
- IV magnesium
- Temporary pacing
- DC cardioversion if unstable
Common Bradycardias
Sinus Bradycardia
- Definition: Sinus rhythm <60 bpm
- ECG findings: Prolonged T-P interval; all waves clearly visible
- Normal in:
- Rest or sleep (parasympathetic tone)
- Elite athletes (↑ stroke volume)
- With negative chronotropes (e.g. β-blockers, digoxin)
- Pathological causes:
- Intrinsic SA-node dysfunction (e.g. ischaemic heart disease, age-related degeneration)
- Cardiomyopathies
- Management:
- Atropine if symptomatic
- +/- Temporary pacing

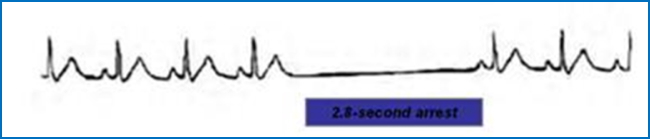
Escape Rhythms (Sinus Arrest / Exit Block)
- Definition: SA-node fails to initiate impulse → AV-node assumes pacing (no P-waves)
- AV-node rate: 40–60 bpm (slower than SA-node)
- Management:
- Cease AV-nodal blockers (e.g. β-blockers, calcium channel blockers, digoxin)
- Consider permanent pacemaker for:
- Complete AV block
- High-grade AV block
- Symptomatic sick sinus syndrome

Brady-Tachy Syndrome
- Definition: Alternating bradycardia and tachycardia due to SA-node instability
- Common in: Elderly patients
- Management:
- Pacemaker insertion

Conduction Blocks
Overview
- Definition: Impaired electrical conduction between atria and ventricles
- Etiology: Ischaemic damage to nodal tissue
- May include:
- Vertical AV conduction blocks
- Lateral conduction blocks (bundle branch blocks)
- May result in: Escape rhythms
AV Conduction Blocks – Degrees
First-Degree AV Block
- PR interval >0.2 sec
- 1:1 P to QRS ratio maintained
- Symptoms: None
- Management: Observation only

Second-Degree AV Block
- Mobitz Type I (Wenckebach):
- Gradually lengthening PR interval → dropped QRS
- Symptoms: Minimal
- Management: Usually none; atropine if symptomatic

Mobitz Type II:
- Intermittent non-conducted P-waves with fixed PR intervals
- Can block for 2+ consecutive beats
- Management: Requires pacemaker

Third-Degree (Complete) AV Block
- No relationship between P-waves and QRS complexes
- Effect: Loss of synchrony → ↓ cardiac output
- Management: Immediate pacemaker insertion

Right Bundle Branch Block (RBBB)
- Right bundle fails to conduct → left bundle depolarises LV first
- Impulse then spreads to RV → delayed RV depolarisation
- ECG: Widened QRS complex
Left Bundle Branch Block (LBBB)
- Left bundle fails to conduct → right bundle depolarises RV first
- Impulse then spreads to LV → delayed LV depolarisation
- ECG: Widened QRS complex

Summary – Arrhythmias
From atrial fibrillation and flutter to complete heart block and torsades de pointes, recognising arrhythmias is central to clinical cardiology. Understand ECG interpretation, rhythm pathophysiology, and the approach to treatment, including when to refer for cardioversion or pacemaker therapy. Want to dive deeper into the cardiovascular system? Explore our Cardiovascular Overview for anatomy, physiology, and pathology summaries.