Table of Contents
Overview
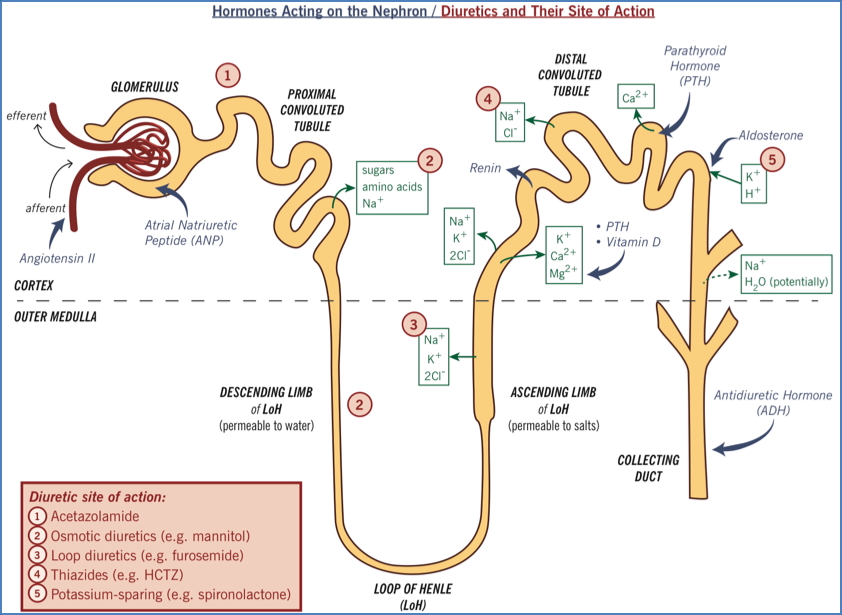
Diuretics are medications that increase urine output by inhibiting sodium reabsorption in various parts of the nephron. This leads to net sodium and water loss, reducing extracellular volume and blood pressure. Their clinical utility spans from managing hypertension and heart failure to treating oedema and preventing renal deterioration. The effectiveness and side effect profile of each diuretic depend on its site of action in the nephron. This page provides a high-yield overview of diuretic classes, their mechanisms, indications, and complications.
Mechanism of Action
- Act at specific nephron segments to inhibit Na⁺ reabsorption → ↑ water excretion
- Effectiveness is proportional to the % of Na⁺ reabsorbed at their site of action:
- Proximal tubule – Osmotic diuretics (∼65%) – most effective
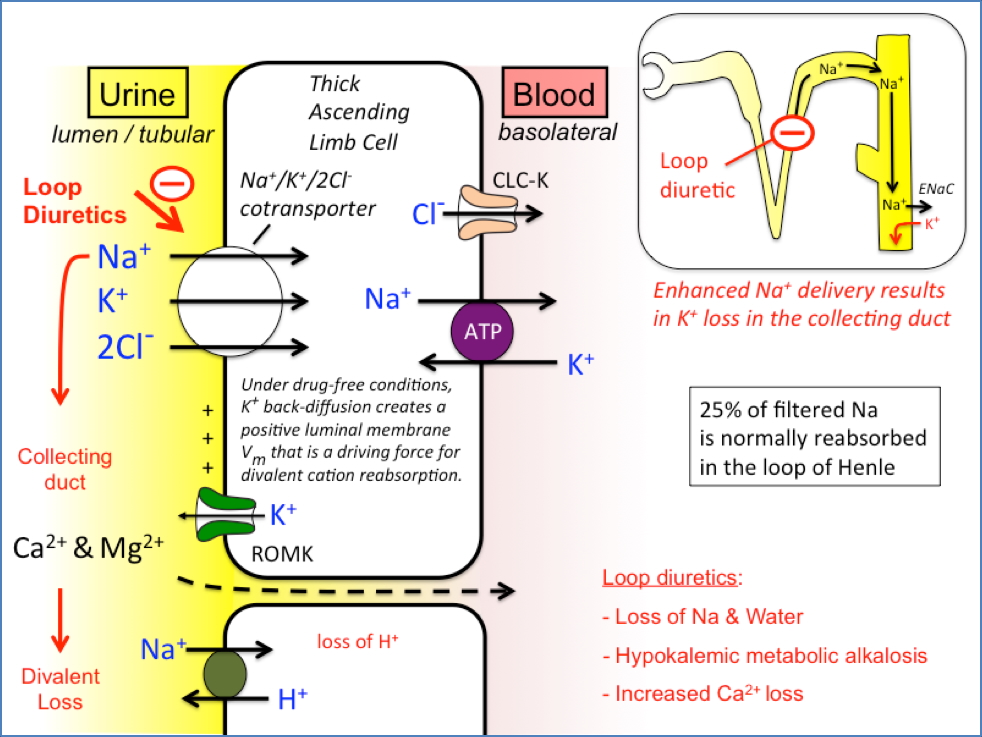
- Loop of Henle – Loop diuretics (∼25%)
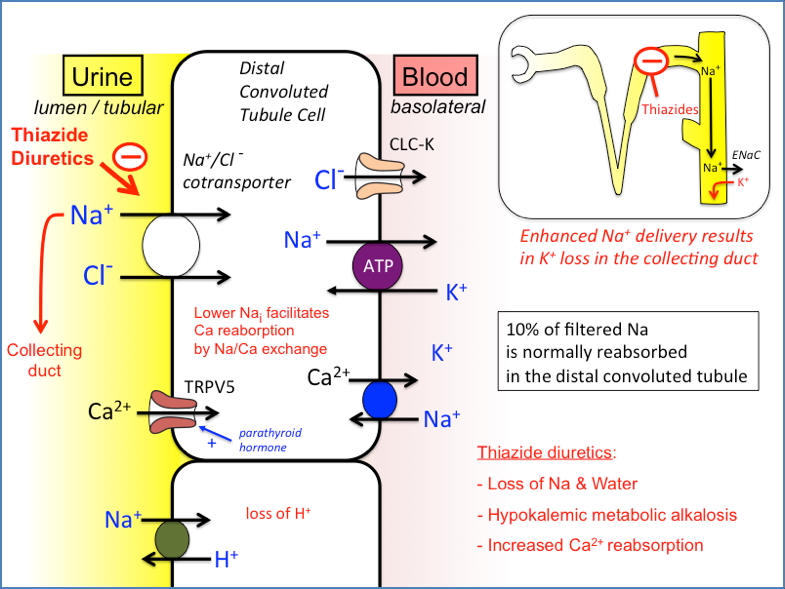
- Distal convoluted tubule – Thiazide diuretics (∼5%)
- Collecting duct – Potassium-sparing diuretics (∼2%)
Indications
- Mild to moderate hypertension
- Heart failure – reduce preload and congestion
- Renal failure – to maintain urine output
- Oedematous states – hepatic cirrhosis, nephrotic syndrome
- Cerebral oedema (osmotic diuretics)
Loop Diuretics
Most powerful; but potassium-wasting
- Site of Action: Thick ascending loop of Henle
- Mechanism: Inhibit the Na⁺/K⁺/2Cl⁻ transporter, impairing counter-current multiplication and water reabsorption
- Indications:
- Acute pulmonary oedema
- Heart failure
- Cirrhotic ascites
- Renal failure
- Side Effects:
- Hypovolaemia, hypotension
- Hypokalaemia → may require potassium supplementation
- Metabolic alkalosis (“concentration alkalosis”)
- Hyperuricaemia → gout
- Ototoxicity (reversible hearing loss)
- Agents:
- Frusemide, Bumetanide, Ethacrynic acid
Thiazide Diuretics
Moderately effective; also potassium-wasting
- Site of Action: Distal convoluted tubule
- Mechanism: Inhibit Na⁺/Cl⁻ symporter, increasing solute concentration in filtrate → H₂O retention in tubule
- Indications:
- First-line for uncomplicated hypertension
- Resistant oedema
- Mild heart failure
- Ascites
- Early chronic renal disease
- Side Effects:
- Hypovolaemia, hypotension
- Hypokalaemia, hyponatraemia
- Hyperglycaemia – can unmask diabetes
- Hyperuricaemia, hypercalcaemia
- Hypomagnesaemia
- Metabolic alkalosis
- Reversible erectile dysfunction
- Agents:
- Chlorothiazide, Chlortalidone
Potassium-Sparing Diuretics
Less effective; used to conserve potassium
1. Epithelial Na⁺ Channel Inhibitors
- Site: Collecting duct
- Mechanism: Block aldosterone-activated Na⁺ channels → reduced Na⁺ reabsorption and K⁺ retention
- Agents: Amiloride, Triamterene
- Side Effects:
- Hyperkalaemia (potentially fatal)
- Avoid in renal failure, with ACE inhibitors or K⁺ supplements
- NSAID interaction
2. Aldosterone Antagonists
- Mechanism: Block aldosterone binding to nuclear receptor → ↓ Na⁺ channel protein expression and ATP-dependent Na⁺ pumping
- Only effective if renin-angiotensin system is active
- Agents: Spironolactone
- Side Effects:
- Hyperkalaemia
- Gynaecomastia, menstrual disturbances, GI upset

Osmotic Diuretics
Mainly used in acute settings
- Site of Action: Proximal tubule and descending limb (freely permeable to H₂O)
- Mechanism: Inert substances (e.g., mannitol) ↑ filtrate osmolality → ↓ H₂O reabsorption
- Indications:
- Cerebral oedema, raised intraocular pressure
- Acute renal failure (to prevent tubular necrosis)
- Side Effects:
- Transient hypervolaemia
- Dilutional hyponatraemia
- May worsen heart failure or cause pulmonary oedema
- Headache, nausea, vomiting
- Agents: Mannitol, Isosorbide, Glycerin

Clinical Notes
- K⁺-wasting diuretics (loop, thiazide) often require potassium monitoring
- K⁺-sparing diuretics are commonly used in combination therapy to balance electrolytes
- Long-term diuretic use should be monitored for electrolyte disturbances and metabolic effects
Summary
Diuretics are a cornerstone of treatment for hypertension, heart failure, oedema, and renal dysfunction. They act at various nephron segments to inhibit sodium and water reabsorption, with potency and side effects dependent on the site of action. For a broader context, see our Renal Overview page.