Table of Contents
Overview – Body Acid-Base Balance
Body acid-base balance is essential for maintaining physiological stability, as even small changes in hydrogen ion (H⁺) concentration can disrupt cellular function. The body generates large amounts of acid daily through metabolic processes, yet arterial pH is tightly regulated around 7.40 by buffer systems, respiratory control, and renal mechanisms. Understanding these defences is vital for diagnosing and managing acid-base disorders in clinical practice.
Acid Production
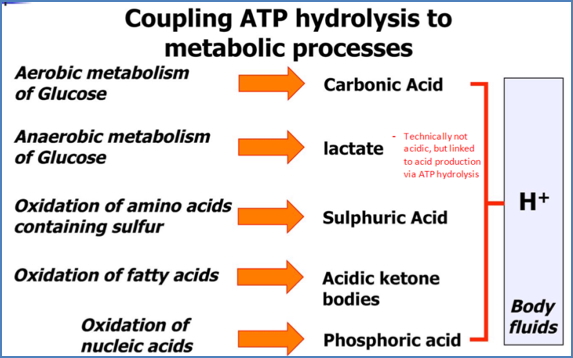
- The body turns over up to 150 moles of H⁺ per day.
- Main sources:
- ATP hydrolysis (aerobic metabolism) → ATP + H₂O → ADP + Pi + H⁺.
- Body turns over ≈40 kg ATP daily.
- Anaerobic metabolism of glucose → lactate.
- Amino acid metabolism (sulphur-containing) → sulphuric acid.
- Fatty acid β-oxidation → acidic ketone bodies.
- Nucleic acid metabolism → phosphoric acid.
- ATP hydrolysis (aerobic metabolism) → ATP + H₂O → ADP + Pi + H⁺.
- Despite high acid production, pH remains stable due to strict regulation.
What is pH?
- pH = negative log of H⁺ concentration: pH = –log[H⁺].
- Acid = proton donor.
- Base = proton acceptor.
Physiological pH Values
- Arterial blood: 7.40 (lethal if <6.9).
- Venous blood: 7.35 (slightly more acidic due to higher PCO₂).
- Urine: 4.5–8.0.
- Stomach: 0.8 (required for digestion).
- Bile: 7.8–8.6 (alkaline to emulsify fats).
Acid-Base Homeostasis
Buffers
- Weak acid + weak base pair resisting pH change.
- pK of a buffer: the pH where acid and base are at 50% dissociation → maximum buffering.
- Isohydric principle: all buffers in a solution equilibrate with the same [H⁺]; all work together when pH changes.
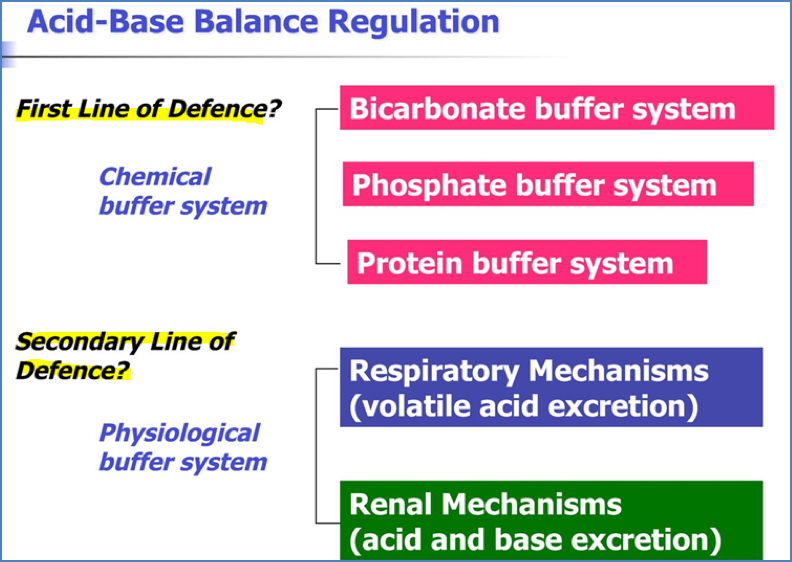
Lines of Defence
- Chemical buffer systems:
- Bicarbonate buffer system.
- Phosphate buffer system.
- Protein buffer system.
- Physiological buffer systems:
- Respiratory regulation.
- Renal mechanisms.
1st Line of Defence: Chemical Buffers
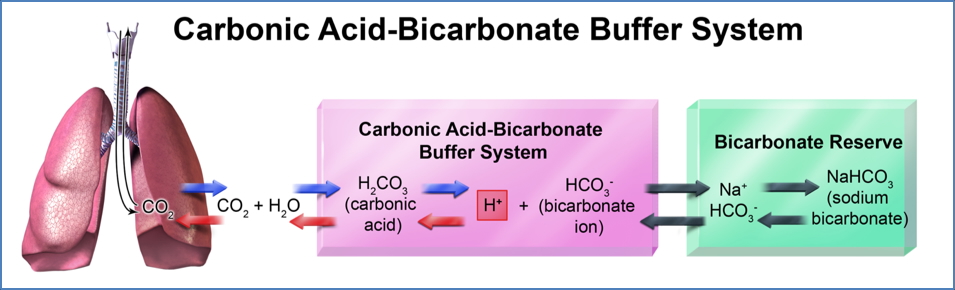
Carbonic Acid–Bicarbonate Buffer
- Most important buffer system, occurs in red blood cells.
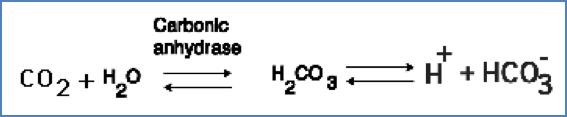
- Carbonic anhydrase catalyses: CO₂ + H₂O ↔ H₂CO₃.
- Linked to respiratory system: blowing off CO₂ ↓[H⁺] → pH rises.
- Normal ratio [HCO₃⁻]:[H₂CO₃] = 20:1 → pH 7.4.
- ↑ HCO₃⁻ or ↓ CO₂ → pH rises.
- ↓ HCO₃⁻ or ↑ CO₂ → pH falls.

Phosphate Buffer System
- Second most important.
- Functions mainly in intracellular fluid:
- H₂PO₄⁻ ↔ H⁺ + HPO₄²⁻.

Protein Buffers
- Intracellular and extracellular proteins act as H⁺ buffers (mainly inside cells).
- Haemoglobin is a key buffer:
- In tissues: Hb releases O₂, binds CO₂ and H⁺.
- In lungs: Hb binds O₂, releasing CO₂ and H⁺.
- Released H⁺ recombines with bicarbonate → H₂CO₃ → H₂O + CO₂ (exhaled).
2nd Line of Defence: Physiological Buffers
Respiratory Control (Short-term)
- CO₂ constantly produced by metabolism, excreted by lungs.
- CO₂ is the main controller of ventilation:
- H⁺ cannot cross the blood-brain barrier; CO₂ crosses, altering CSF pH.
- ↑ PCO₂ → ↑ ventilation rate & depth (e.g. exercise).
- ↓ PCO₂ → ↓ ventilation rate & depth (e.g. after hyperventilation).
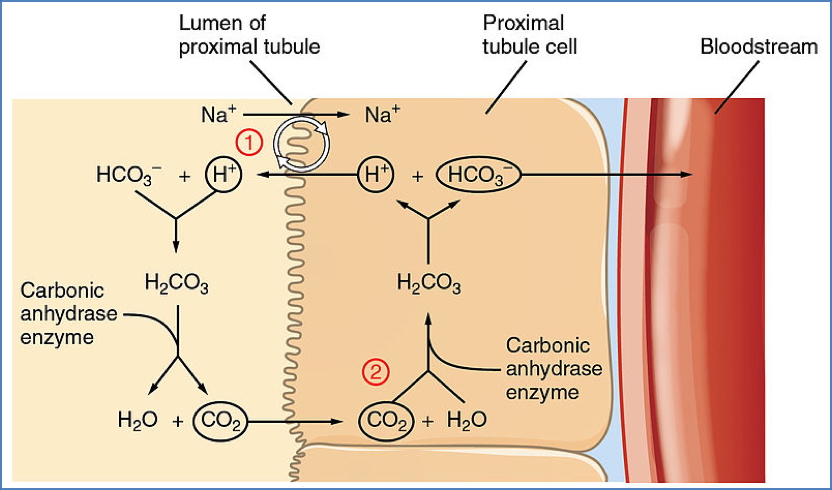
Renal Control (Long-term)
- Kidneys regulate acid-base by excreting acidic or alkaline urine.
- Mechanism:
- HCO₃⁻ filtered → reabsorbed via combination with H⁺.
- H⁺ excreted by combining with phosphate or ammonia.
- Net effect: recovery of bicarbonate into blood, excretion of H⁺ into urine.
Metabolic vs Respiratory Disturbances
Metabolic
- Acidosis: ↓ HCO₃⁻ (renal failure, lactic acidosis, ketoacidosis).
- Alkalosis: ↑ HCO₃⁻ (vomiting, bicarbonate retention).
Respiratory
- Acidosis: ↑ PCO₂ (hypoventilation, alveolar disease).
- Alkalosis: ↓ PCO₂ (hyperventilation).

Compensatory Mechanisms
- Metabolic disturbances → compensated by respiratory changes.
- Respiratory disturbances → compensated by renal adjustments.
- Example: metabolic acidosis triggers hyperventilation to reduce CO₂.
- Exception: in metabolic acidosis, chemoreceptors respond directly to low blood pH because CO₂ is already reduced.
Anion Gap
- Equation: Anion Gap = Na⁺ – (Cl⁻ + HCO₃⁻).
- Reflects unmeasured anions (e.g. lactate, ketones).
- Normal anion gap acidosis: loss of HCO₃⁻ compensated by ↑ Cl⁻ → hyperchloraemic acidosis.
- High anion gap acidosis: accumulation of unmeasured acids (lactate, ketoacids).
Summary – Body Acid-Base Balance
Body acid-base balance is maintained through buffer systems, respiratory regulation, and renal excretion, despite large daily H⁺ loads. Key defences include the bicarbonate buffer, phosphate and protein systems, and compensatory responses to metabolic or respiratory disturbances. The anion gap provides an important diagnostic clue in metabolic acidosis. For broader context, see our Respiratory Overview page.