Table of Contents
Overview – Lung Cancer
Lung cancer is the leading cause of cancer-related mortality worldwide. It encompasses a group of malignant tumours arising primarily from the epithelium of the bronchi and lung parenchyma. The disease is broadly classified into small cell and non-small cell lung cancers, with distinct pathological and clinical features. Smoking remains the most significant risk factor. Symptoms may be subtle until late stages, making early recognition and staging critical. This page outlines the classification, pathogenesis, clinical features, investigations, and management of lung cancers.
Definition
Lung cancer refers to malignant neoplasms originating in the respiratory epithelium of the lungs and bronchial tree, with classification into small cell and non-small cell subtypes.
Classification
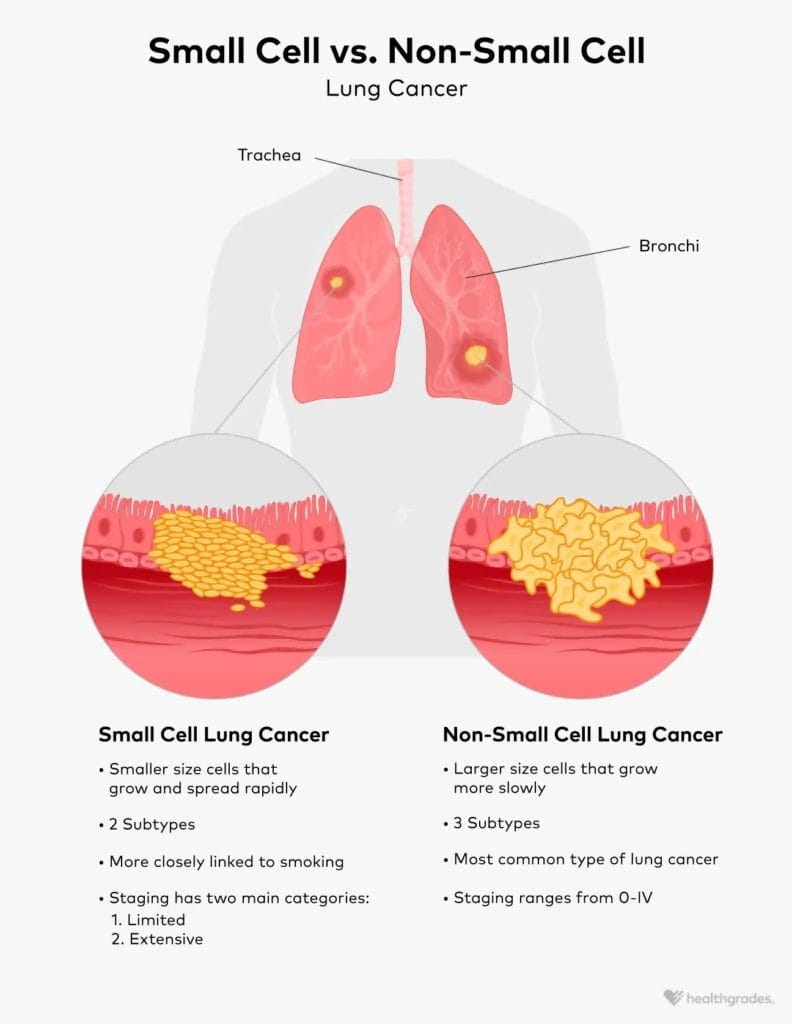
Small Cell Lung Carcinoma (SCLC)
- Accounts for 20% of cases
- Strongly associated with smoking
- Centrally located
- Highly aggressive, poorly demarcated
- Early metastasis
- Treatment: Chemotherapy (not surgical)
Non-Small Cell Lung Carcinoma (NSCLC)
Accounts for 80% of cases and includes:
- Squamous Cell Carcinoma
- Associated with smoking
- Typically central
- Well-demarcated, mildly aggressive
- Treatment: Surgery preferred
- Adenocarcinoma
- Most common in non-smokers and females
- Typically peripheral
- Well-demarcated, mildly aggressive
- Treatment: Surgery
- Large Cell Anaplastic Carcinoma
- More common in males
- Usually central
- Poorly differentiated
- Treatment: Surgery
Aetiology
- Smoking (major risk factor; ~90% of cases)
- Occupational exposures: asbestos, coal dust, radon
- Ionising radiation
- Air pollution
- Genetic predisposition
Pathogenesis
Repeated exposure to carcinogens (e.g., tobacco smoke) causes:
- Metaplasia – normal ciliated epithelium replaced by squamous epithelium
- Dysplasia – pre-cancerous cellular changes
- Neoplasia – unregulated growth
- Invasion – spread beyond the basement membrane
Morphology
- Central or peripheral masses
- Poorly demarcated or lobulated tumours
- May infiltrate surrounding structures (e.g., pleura, pericardium, chest wall)
- Potential for cannonball metastases on chest imaging
Clinical Features
Common Symptoms
- Persistent dry cough
- Dyspnoea
- Haemoptysis
- Chest pain
- Weight loss
Local Complications
- Airway obstruction → Pneumonia, atelectasis, bronchiectasis
- Pleural involvement → Pleural effusion
- Pericardial involvement → Pericardial effusion, tamponade
- Nerve involvement:
- Recurrent laryngeal → Hoarseness
- Phrenic nerve → Diaphragmatic paralysis
- Brachial plexus → Pancoast syndrome (shoulder pain, hand weakness)
- Sympathetic ganglia → Horner’s syndrome
Paraneoplastic Syndromes
Primarily associated with SCLC:
- SIADH – Hyponatraemia due to ↑ADH
- Cushing’s Syndrome – Due to ectopic ACTH
- Carcinoid Syndrome – ↑Serotonin → flushing, diarrhoea
- Hypertrophic Pulmonary Osteoarthropathy (HPOA) – Clubbing, joint pain
Pancoast Tumours
- Apical lung cancers that invade adjacent structures
- Horner’s Syndrome:
- Ptosis
- Miosis
- Anhidrosis
- Enophthalmos
- May cause brachial plexus compression → arm pain, muscle wasting
Investigations
- Imaging: CXR, CT chest, PET scan, bone scan
- Histology: Sputum cytology, bronchoscopy with biopsy, fine needle aspirate
- Tumour markers: For monitoring response (not diagnostic)
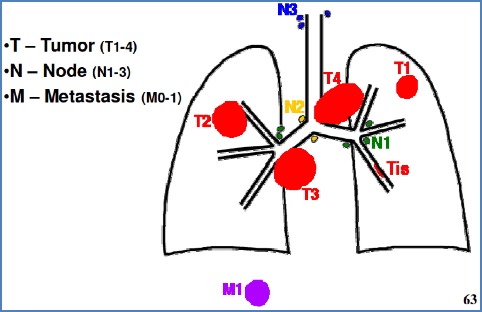
- Staging: TNM classification (Tumour, Node, Metastasis)
Management
NSCLC
- Surgery: Lobectomy or pneumonectomy
- Radiotherapy: Curative in non-surgical candidates
- Chemotherapy: Adjuvant or for unresectable disease
SCLC
- Chemotherapy: Mainstay of treatment
- Radiotherapy: Often adjunctive
Prognosis
- Overall 5-year survival is low (~15%)
- Prognosis depends on:
- Histological subtype
- Stage at diagnosis
- Response to treatment
Summary – Lung Cancer
Lung cancer is a common cause of cancer death worldwide and includes small cell and non-small cell subtypes, each with distinct behaviour and treatment. It often presents late with cough, weight loss, or haemoptysis, and may cause airway obstruction or paraneoplastic syndromes. Management depends on tumour type and stage, with surgery used in NSCLC and chemotherapy preferred for SCLC. Accurate staging is essential. For more on related pulmonary conditions, visit the Respiratory Overview page.