Table of Contents
Overview – Meningitis
Meningitis is an acute inflammation of the meninges with potentially life-threatening consequences, particularly when bacterial. It is commonly caused by bacterial or viral pathogens and can rapidly progress to cerebral oedema, raised intracranial pressure, and sepsis. Clinical recognition, empirical treatment, and timely CSF analysis are vital for optimal outcomes. This article outlines the causes, classical signs of meningism, diagnostic red flags, and the CSF interpretation framework essential for clinical practice in final-year medicine.
Definition
Inflammation of the meninges (pia, arachnoid, dura mater), usually due to bacterial, viral, or less commonly fungal or mycobacterial infection.
Aetiology
Bacterial (Septic) Meningitis
- Adults: Neisseria meningitides (meningococcus) – vaccine preventable (A & C)
- Children: Haemophilus influenzae – HIB vaccine preventable
- Neonates: Group B Streptococcus, E. coli
Viral (Aseptic) Meningitis
Chronic Meningitis
- Miliary tuberculosis
Fungal Meningitis
- Usually in immunocompromised patients
Pathophysiology
- Infection of the meninges → Inflammatory cytokine release → Cerebral oedema
- ↑Intracranial pressure → vomiting, headache, drowsiness
- Meningococcaemia may trigger thrombocytopenia → petechial rash → DIC
Morphology
- Bacterial: Purulent exudate under the meninges
- Viral: No pus
- Engorgement of meningeal vessels
Clinical Features
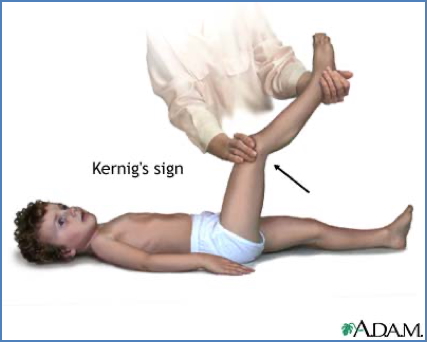
Meningism (Classic Triad)
- Neck Stiffness
- Brudzinski’s sign (neck flexion → hip/knee flexion)
- Kernig’s sign (hip flexion → painful knee extension)
- Photophobia
- Headache

Other Symptoms
- Fever, vomiting
- Nausea, malaise
- Papilloedema (<1%)
- Irritability, poor feeding (infants)
- Altered consciousness (late)
Aetiology-Specific Clues
- Non-blanching maculopapular rash → Neisseria meningitidis
- CSF rhinorrhoea/otorrhoea → Suggests pneumococcus, HiB, or Strep due to basal skull fracture

Investigations
Immediate Actions
- Blood cultures BEFORE antibiotics
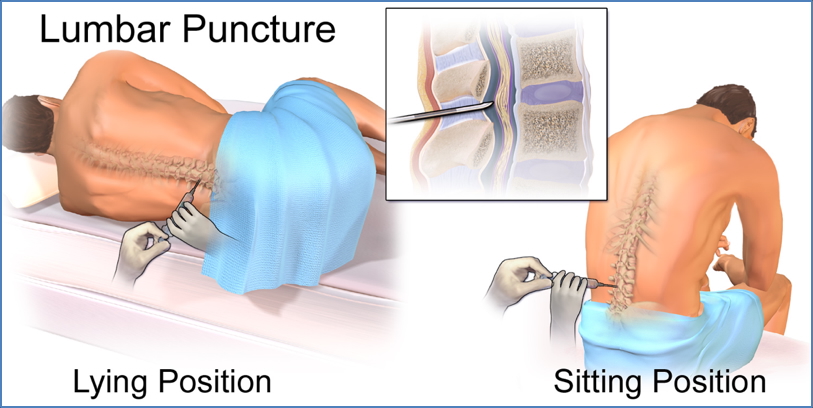
Lumbar Puncture (L3-L5) for CSF Analysis
Contraindications (signs of ↑ICP):
- Papilloedema
- Cushing’s response (↑BP, ↓HR, irregular breathing)
- Unreactive pupils
Risk: Coning (brainstem herniation) → potentially fatal
CSF Sample Breakdown
- Tube 1: Serology / PCR
- Tube 2: Biochemistry (protein, glucose)
- Tube 3: Bacteriology (gram stain & culture – most important)
CSF Interpretation
| Feature | Normal | Bacterial Meningitis | Viral Meningitis |
|---|---|---|---|
| CSF Pressure | Normal | Normal–raised | Normal–raised |
| White Cell Count | Normal | ↑ Polymorphs | ↑ Lymphocytes |
| Glucose | Same as serum | ↓ (bacteria consume glucose) | Normal |
| Protein | Normal | ↑ | ↑ |
| Gram Stain | None | Bacteria present | Nil (aseptic) |
Management
Bacterial Meningitis
Medical emergency – treat on clinical suspicion
- Blood cultures first
- Empirical IV antibiotics immediately
- IV Benzylpenicillin G or IV Ceftriaxone (crosses BBB)
- Add corticosteroids (e.g. IV dexamethasone) to reduce CNS inflammation
- Fundoscopy (for papilloedema) before LP
- Post-exposure prophylaxis for close contacts:
- Rifampicin, Ceftriaxone, or Ciprofloxacin
Viral Meningitis
- Typically self-limiting
- Supportive care
Complications
Acute
- Encephalitis
- Cerebral infarction
- Brain herniation
- Cerebral oedema
- Waterhouse-Friderichsen syndrome (adrenal infarction, DIC)
Late
- Brain abscess
- Subdural empyema
- Epilepsy
- Leptomeningeal fibrosis → hydrocephalus
Differential Diagnosis
- Encephalitis
- Brain abscess
- Subarachnoid haemorrhage
- Intracranial tumour
- Migraine (with photophobia)
- Acute febrile illness with myalgia (e.g. influenza)
Summary – Meningitis
Meningitis is an urgent neurological condition that presents with meningism, fever, and headache, and can rapidly progress to cerebral oedema, herniation, or death without timely management. Diagnosis relies on clinical suspicion, lumbar puncture, and CSF analysis. Bacterial meningitis requires immediate empirical antibiotics. For a broader context, see our Nervous System Overview page.