Table of Contents
Overview – Helicobacter Pylori
Helicobacter pylori is a spiral-shaped, Gram-negative bacterium that colonises the human stomach and duodenum. With a global distribution and high prevalence in patients with peptic ulcer disease (PUD), H. pylori is now recognised as a Class I carcinogen due to its role in chronic gastritis and gastric adenocarcinoma. It thrives in the acidic gastric environment by producing urease and demonstrates several adaptations and pathogenicity factors that contribute to mucosal inflammation, ulceration, and carcinogenesis.
Microbiology & Characteristics
- Gram-negative, spiral-shaped (spirochete)
- Microaerophilic (low oxygen tolerance)
- Urease-producing (neutralises stomach acid with ammonia)
- Metabolically fastidious – grows slowly in culture
- Transmission:
- Oral–oral
- Faecal–oral
- Vertical (parent to child)
- Colonisation sites:
- Duodenum (most common)
- Gastric antrum
- Gastro-oesophageal junction
- Class I carcinogen (via chronic inflammation and ROS exposure)
Pathogenesis
Gastric Ulcer
- Colonisation of gastric corpus
- → Gastritis → Epithelial damage → Ulcer
- → ↓D-Cells (somatostatin) → ↓Inhibition of G-Cells
- → ↑Gastrin → ↑Histamine → ↑Parietal cell acid secretion
Duodenal Ulcer
- Colonisation of gastric antrum
- → ↓D-Cells → ↑Gastrin → ↑Acid
- → Duodenal metaplasia + inflammation → Duodenitis → Ulcer
Adaptations & Virulence
Hostile Environment Adaptations
- Utilises carbohydrates (e.g. glucose)
- Pyruvate & fumarate metabolic pathways
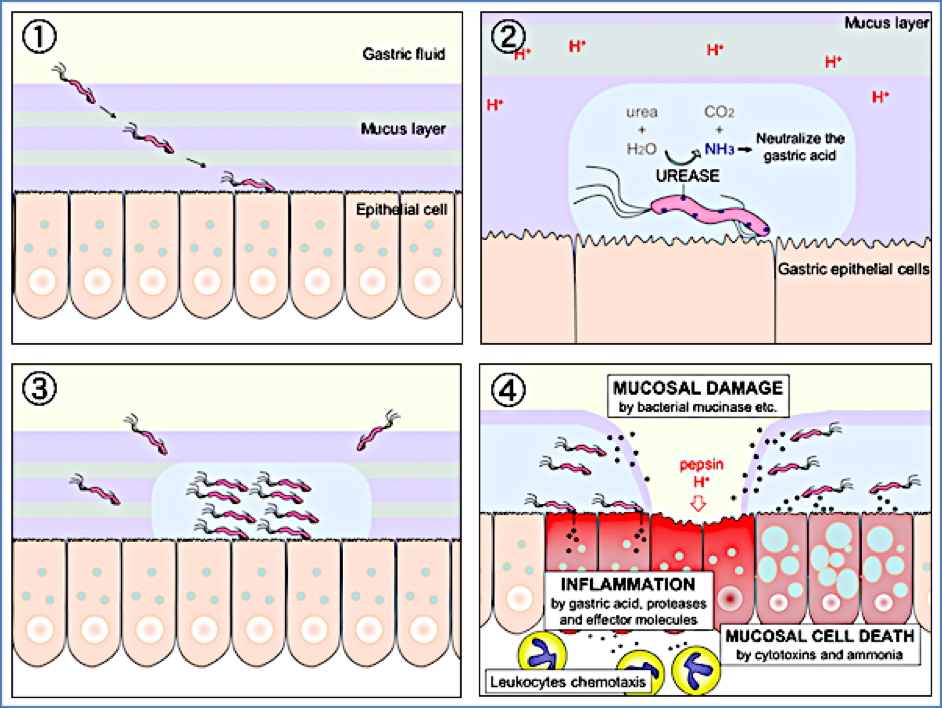
- Urease activity: urea → ammonia + bicarbonate (↑ local pH)
Pathogenicity Factors
- Urease → pH neutralisation
- Flagella → motility in mucus
- Adhesins → epithelial attachment
- Type-IV secretion system (e.g. CagA protein):
- Disrupts tight junctions
- ↑COX-2 → ↑Prostaglandins → inflammation
- Triggers inflammatory cytokines
Clinical Features
- Global prevalence; higher in:
- Developing countries
- Elderly
- Low socioeconomic status
- Chronic infection if untreated → lifetime colonisation
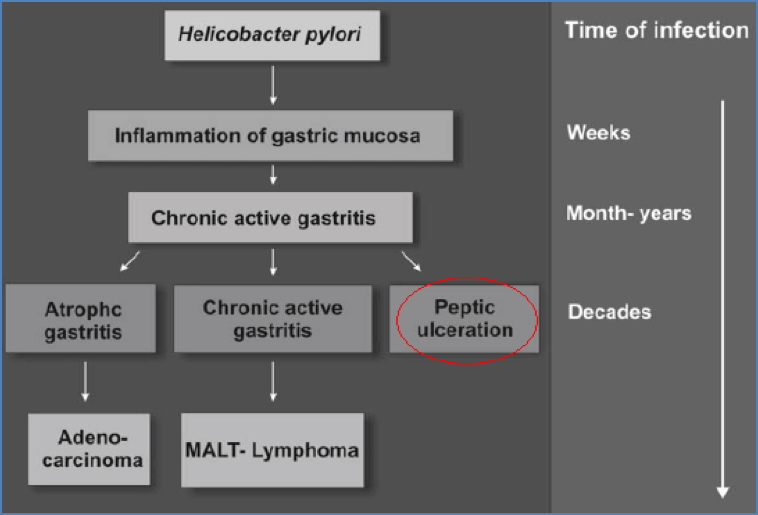
- Associated diseases:
- Gastritis
- Peptic ulcer disease
- Gastric cancer (adenocarcinoma)
- MALT lymphoma
Diagnosis
- Gastric biopsy:
- Histology
- Culture
- Serology:
- Antibody detection (e.g. via gel electrophoresis)
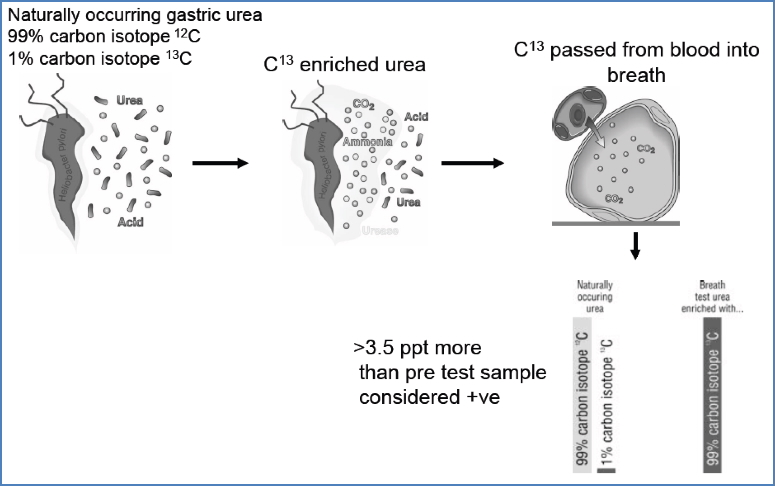
- C13 Urea Breath Test:
- C13-labelled urea → cleaved by urease
- Exhaled CO₂ with C13 indicates infection
- Faecal antigen test – useful for active infection
Management
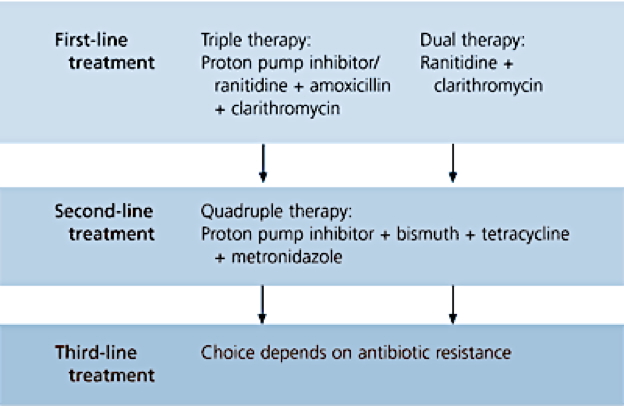
First-Line Therapy
- Triple therapy:
- PPI (e.g. Omeprazole)
- Clarithromycin
- Amoxicillin or Metronidazole
Adjunct
- Bismuth-containing preparations:
- Directly toxic to H. pylori
- Inhibits adhesion and proteolysis
- PPI therapy:
- ↓ gastric acidity
- Enhances healing
Cure rate <80%; rising antibiotic resistance driving vaccine research
Vaccine Research
- 100+ antigens identified
- Promising in animal studies, but poor human efficacy
- CD4+ T-cells involved; antibody response insufficient
- Post-vaccine gastritis is a concern
- No safe, effective human vaccine currently available
Summary – Helicobacter Pylori
Helicobacter pylori is a highly adapted, globally prevalent bacterium responsible for gastritis, peptic ulcer disease, and gastric cancer. Its unique survival mechanisms and potent virulence factors make eradication critical. Diagnosis involves non-invasive tests like the C13 urea breath test, and management relies on triple therapy. Despite ongoing research, a human vaccine remains elusive. For more information, see our Gastrointestinal Overview page.