Table of Contents
Overview – The Rheumatological Examination
The rheumatological examination is a core clinical skill essential for evaluating joint, connective tissue, and systemic autoimmune diseases. It involves a head-to-toe assessment to detect key signs of inflammatory arthritis (e.g. rheumatoid arthritis), connective tissue disorders (e.g. systemic lupus erythematosus and scleroderma), metabolic joint disease (e.g. gout), and seronegative spondyloarthropathies. Recognising deformities, rashes, nodules, and synovitis early is vital to ensuring timely diagnosis, improving quality of life, and preventing irreversible joint damage.
Preparation
- Introduce yourself, explain the examination, and gain consent
- Wash hands and ensure full exposure of limbs and face where appropriate
- Patient seated or lying comfortably depending on joint/system being examined
General Inspection
- Cushingoid appearance (moon face, central obesity): Long-term corticosteroid use
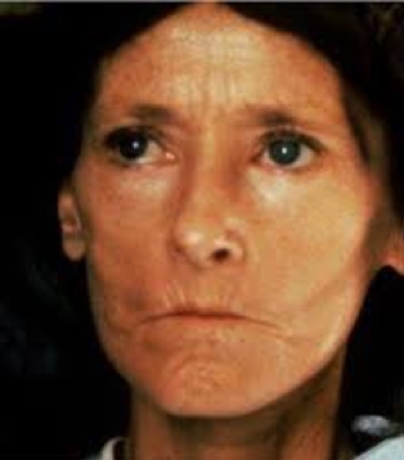
- Bird-like facies: Seen in scleroderma
- Weight loss: Common in autoimmune disease
- Butterfly malar rash and hair loss: Systemic lupus erythematosus (SLE)


Hands
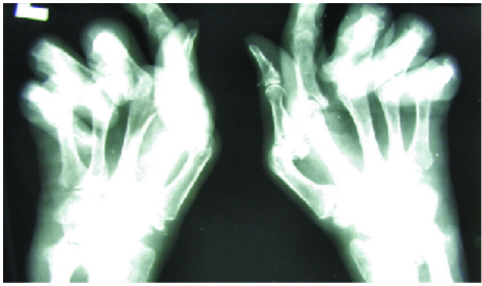
Rheumatoid Arthritis (RA)
- Symmetrical PIP joint synovitis (red, swollen, tender)
- Ulnar deviation
- MCP joint subluxation
- Z-deformity of thumb
- Swan neck and boutonnière deformities
- Small muscle wasting (thenar and hypothenar eminences)
- Palmar tendon crepitus
- Splinter haemorrhages (vasculitis)
- Carpal tunnel signs (e.g. inverse prayer test)

Osteoarthritis (OA)
- Heberden’s nodes (DIP joints)
- Bouchard’s nodes (PIP joints)

Gout
- Gouty tophi in finger joints

Scleroderma (CREST)
- Calcinosis: Calcific nodules on fingers
- Raynaud’s phenomenon: Triphasic colour change
- Sclerodactyly: Tapered, stiff fingers
- Telangiectasia: Dilated vessels on skin

Reiter’s Syndrome
- Syphilitic-like palmar and plantar lesions

Arms
- Rheumatoid nodules: Elbows
- Gouty tophi: Elbows, wrists
- Psoriatic plaques: Extensor surfaces (elbows, knees)

Face
Rheumatoid Arthritis
- Dry eyes & mouth (Sjögren’s syndrome)
- Cataracts (steroid use)
- Conjunctival pallor (NSAID-induced anaemia)
- Parotid gland enlargement (Sjögren’s)
- Mouth ulcers, gum hypertrophy (methotrexate toxicity)
- TMJ crepitus
Ankylosing Spondylitis
- Acute iritis
Reiter’s Syndrome
- Conjunctivitis
- Uveitis/Iritis
Gout
- Tophi on ear helix
Neck
- Cervical lymphadenopathy: SLE, RA
Chest
Rheumatoid Arthritis
- Spinal tenderness
- Pleural effusions
- Pericardial rub
- Aortic regurgitation murmur
Ankylosing Spondylitis
- ↓ Spinal ROM
- ↓ Chest expansion
- Postural changes: Lordosis, kyphosis
- Sacroiliac joint tenderness
- Aortic regurgitation murmur
Abdomen
- Hepatosplenomegaly: Seen in RA and SLE
Genital Exam (if appropriate)
Reiter’s Syndrome
- Urethral discharge, balanitis, prostatitis
Legs
Rheumatoid Arthritis
- Quadriceps wasting
- Valgus knee deformity
- Knee crepitus
- Baker’s cysts (popliteal fossa)
- Peripheral neuropathy (e.g. foot drop)
Ankylosing Spondylitis
- Achilles tendonitis
- Plantar fasciitis
Gout
- Tophi in big toe (75% of cases)
- Tophi in Achilles tendon
Feet
Rheumatoid Arthritis
- MTP swelling and subluxation
- Claw toe deformity
- Foot drop
- Achilles tendon nodules
Reiter’s Syndrome
- Sausage toes (dactylitis)
- Achilles tendonitis, plantar fasciitis
- Palmar/plantar hyperkeratotic lesions
Summary – The Rheumatological Examination
The rheumatological examination is essential for identifying inflammatory, autoimmune, metabolic, and seronegative arthropathies. It requires careful inspection of hands, joints, skin, and systemic features. Recognition of hallmark signs—like swan neck deformities, tophi, malar rash, or sclerodactyly—enables early diagnosis and optimises long-term management. For a broader context, see our Clinical Skills Overview page.