Table of Contents
Overview – Transitional Cell Carcinomas
Transitional cell carcinomas (TCC), also known as urothelial carcinomas, arise from the transitional epithelium that lines much of the urinary tract, including the renal pelvis, ureters, bladder, and proximal urethra. The bladder is the most common site. TCCs are strongly associated with smoking and chronic bladder irritation, often presenting with painless haematuria. Given their potential to cause urinary obstruction and their high recurrence rate, timely diagnosis and multidisciplinary management are crucial. This article summarises key facts about transitional cell carcinomas for final-year medical students.
Definition
Transitional cell carcinoma is a malignant tumour of the urothelial (transitional) epithelium, which lines the urinary tract. It most commonly affects the bladder, but may occur anywhere from the renal pelvis to the proximal urethra.
Aetiology
Risk Factors
- Smoking – most significant modifiable risk
- Chronic cystitis – e.g., due to long-term catheter use or bladder stones
- Male sex
- Older age
Morphology / Pathophysiology
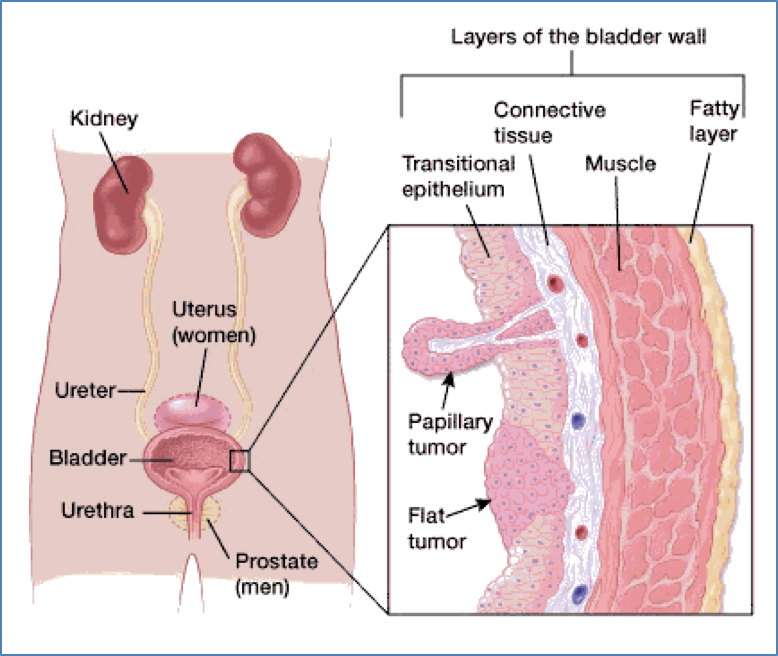
- Arises from transitional epithelium lining the urinary tract
- Most commonly originates in the bladder
- May involve:
- Papillary projections into the urinary lumen
- Spread along the urinary tract (renal pelvis → ureters → bladder)
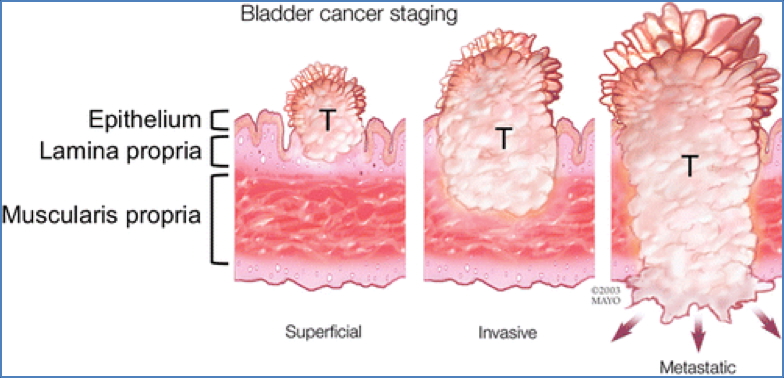
- Advanced disease can obstruct urinary flow:
- Bladder outlet obstruction
- Hydronephrosis (due to ureteral blockage)
2. Daniel B. Green, et al; RadioGraphics 2019 39:1, 80-94; https://pubs.rsna.org/doi/full/10.1148/rg.2019180014
Clinical Features
- Painless haematuria – classic presenting symptom
- Lower urinary tract symptoms (LUTS) if obstruction present
- Signs of bladder outlet obstruction may include:
- Difficulty urinating
- Intermittent flow
- Flank pain (if upper tract obstructed → hydronephrosis)
Investigations
- Urine MCS (microscopy, culture, sensitivity)
- May reveal malignant cells
- Further work-up (not listed but important to mention for students):
- Cystoscopy – direct visualisation and biopsy
- CT urogram – for upper tract involvement and staging
- Urinary cytology – for high-grade or carcinoma in situ lesions
Management
- Surgical resection – including transurethral resection or cystectomy depending on tumour location and staging
- Chemotherapy – often used in muscle-invasive or metastatic disease
- Radiotherapy – adjunctive in selected cases or bladder preservation protocols
Complications
- Hydronephrosis from ureteral obstruction
- Local invasion into surrounding tissues
- Metastasis – to lymph nodes, liver, lungs, and bones
- High recurrence rate, particularly for bladder TCCs
Differential Diagnosis
- Renal cell carcinoma (especially if haematuria present)
- Squamous cell carcinoma of the bladder (rare, often schistosomiasis-related)
- Urethral strictures or benign prostatic hyperplasia (for obstructive symptoms)
- Urinary tract infection or nephrolithiasis
Summary – Transitional Cell Carcinomas
Transitional cell carcinomas are malignant tumours arising from the urothelial lining of the urinary tract, most commonly in the bladder. They typically present with painless haematuria and may lead to obstructive uropathy such as hydronephrosis. Risk factors include smoking and chronic cystitis. Management involves surgery with adjunctive chemotherapy or radiotherapy as needed. For a broader context, see our Renal Overview page.