Table of Contents
Overview
Renal cell carcinoma (RCC) is the most common type of kidney cancer in adults, accounting for approximately 90% of all renal malignancies. Often presenting silently until late in its course, RCC typically arises from the proximal convoluted tubules and most commonly manifests as painless haematuria. Understanding the clinical features, pathogenesis, complications, and management of RCC is essential for final-year medical students, especially given its association with paraneoplastic syndromes and potential for vascular invasion. This article covers the core aspects of renal cell carcinoma relevant to exam preparation and clinical practice.
Definition
Renal cell carcinoma (RCC), often referred to as “clear cell carcinoma,” is a malignant tumour originating from the renal tubular epithelium, particularly the proximal convoluted tubules. It is the most prevalent primary renal malignancy in adults.
Aetiology
Genetic
- Von Hippel-Lindau (VHL) gene mutation is strongly implicated in RCC development.
Risk Factors
- Smoking
- Obesity
- Chronic analgesic (NSAID) abuse
- Male sex (M:F ratio = 3:1)
- Age > 50 years
Morphology / Pathophysiology
- Originates from epithelial cells of the proximal convoluted tubules.
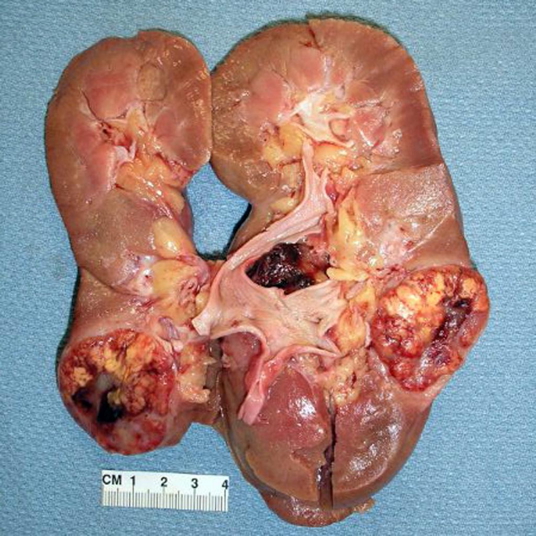
- Gross pathology:
- Enlarged kidney
- Yellowish-orange tumour (due to high lipid content)
- Well-demarcated and encapsulated appearance
- May show haemorrhage and necrosis
- Possible invasion into the renal vein, a hallmark of aggressive disease
Clinical Features
- Most common primary renal malignancy
- Typically asymptomatic in early stages
- Classical triad (seen in ~10%):
- Painless haematuria (most common symptom)
- Flank pain
- Palpable abdominal or lower back mass
- Systemic symptoms:
- Fever
- Weight loss
- Night sweats
- Weakness and malaise
- Renal vein invasion may cause:
- Ipsilateral varicocoele (especially on the left)
Investigations
- CT abdomen with contrast:
- First-line for diagnosis and staging
- Can identify local invasion and metastasis
Management
- Nephrectomy (partial or radical), depending on tumour size and spread
- Chemotherapy is generally limited in effectiveness
- Immunomodulatory therapy may include:
- Interferon-alpha (IFN-α)
- Interleukin-2 (IL-2)
- Monoclonal antibodies (e.g., anti-VEGF therapies)
Complications
Metastasis
- Common sites: lungs, bones, liver, and brain
- Primarily via haematogenous spread, particularly through the renal vein
Paraneoplastic Syndromes
- ↑ Parathyroid hormone-related peptide → Hypercalcaemia
- May result in nephrolithiasis (calcium stones)
- ↑ Erythropoietin (EPO) → Polycythaemia
- ↑ Adrenocorticotropic hormone (ACTH) → Cushing syndrome
Prognosis
- Overall 5-year survival ~60%, but significantly lower for metastatic disease
Differential Diagnosis
- Transitional cell carcinoma (urothelial carcinoma of renal pelvis)
- Renal oncocytoma
- Angiomyolipoma
- Wilms tumour (children)
- Metastatic lesions to the kidney
Summary
Renal cell carcinoma is the most common renal malignancy in adults, originating from the proximal convoluted tubules. It often presents late with features such as painless haematuria, flank pain, and abdominal masses. Key complications include metastatic spread and a range of paraneoplastic syndromes. Management is primarily surgical, with adjuvant immunotherapy where appropriate. For a broader context, see our Renal Overview page.