Table of Contents
Overview – Acute Renal Failure
Acute renal failure (ARF), now more commonly referred to as acute kidney injury (AKI), is defined as a rapid loss of renal function leading to impaired fluid, electrolyte, and metabolic homeostasis. ARF is classified based on the anatomical site of dysfunction—pre-renal, intra-renal, and post-renal. Early identification and classification are crucial for effective intervention and prevention of permanent damage.
Classification of Acute Renal Failure
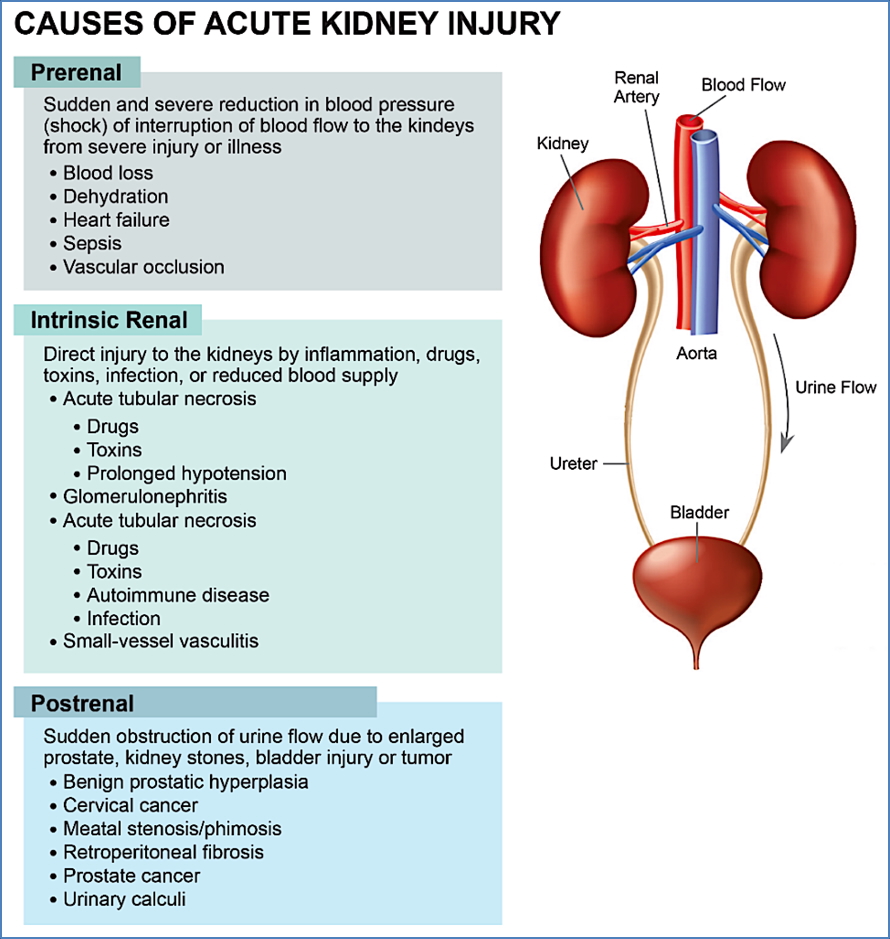
1. Pre-Renal Failure (↓ Perfusion)
Occurs before blood reaches the nephron, due to reduced renal perfusion.
Examples:
- Hypovolaemia (e.g. blood loss, dehydration)
- Heart failure (↓ cardiac output)
- Renal artery stenosis or embolism
- Sepsis
2. Intra-Renal Failure (Structural Kidney Damage)
Results from direct injury to the renal parenchyma (glomeruli, tubules, interstitium, or vasculature).
Examples:
- Acute glomerulonephritis
- Acute tubular necrosis (e.g. drugs, toxins, prolonged hypotension)
- Interstitial nephritis (e.g. SLE)
- Vascular causes (e.g. polyarteritis nodosa, vasculitis)
3. Post-Renal Failure (Outflow Obstruction)
Results from urinary tract obstruction distal to the kidney.
Examples:
- Ureteric or bladder cancer
- Prostatic enlargement (BPH, cancer)
- Cervical cancer
- Blood clots
- Bilateral renal calculi
- Accidental surgical ligation
Common Clinical Features
- Uraemia: fatigue, anorexia, nausea, headache, vomiting
- Hyperkalaemia: brady-arrhythmias, ECG changes
- Fluid overload: peripheral oedema, pulmonary oedema, possibly cardiac tamponade
- Oliguria or anuria
- Haematuria: painless (malignancy), painful (stones)
- Flank pain: more typical in ischaemic or inflammatory intra-renal injury
Pathophysiological Complications of Renal Failure
Think of the kidney’s normal functions and what happens when they are lost:
- Acid–base balance: metabolic acidosis
- Electrolyte balance: hyperkalaemia, hyponatraemia
- Fluid regulation: overload, oedema
- Erythropoietin deficiency: anaemia
- Renin-angiotensin disruption: secondary hypertension
- Calcium-phosphate imbalance: osteoporosis, secondary hyperparathyroidism
- Toxin accumulation: uraemia (neurotoxicity, nausea, pruritus)
- Reduced urine output
Diagnostic Investigations
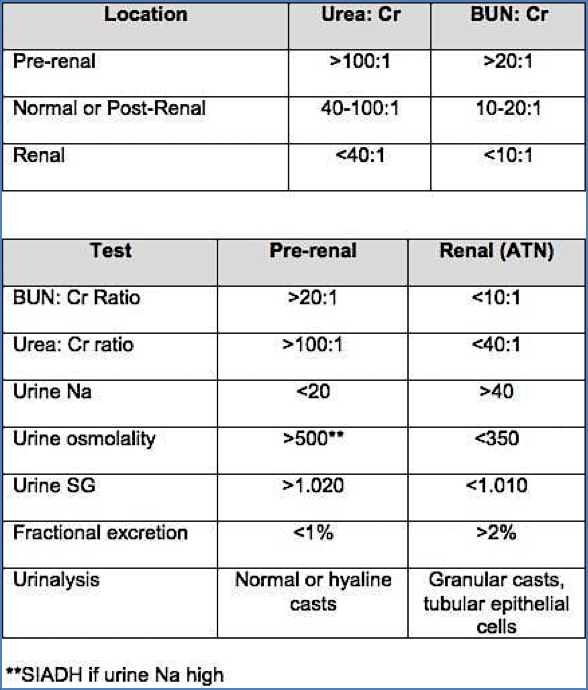
Blood Urea:Creatinine Ratio (U:Cr)
Useful in distinguishing between causes:
- Normal ratio: ~40:1 – 100:1
- High ratio: suggests pre-renal or post-renal cause
- Low ratio: indicates intra-renal failure (e.g. ATN)
Note: Both absolute urea and creatinine levels are raised in all types of renal failure.
Urine Protein:Creatinine Ratio (Pr:Cr)
Assesses the degree of proteinuria:
- 30–300 mg/g: microalbuminuria
- >300 mg/g: proteinuria (macroalbuminuria)
- >3000 mg/g: nephrotic-range proteinuria
Summary – Acute Renal Failure
Acute renal failure refers to a rapid decline in kidney function, commonly classified as pre-renal, intra-renal, or post-renal based on the location and cause of the insult. Clinical features include uraemia, electrolyte disturbances like hyperkalaemia, and fluid overload. Key investigations such as the urea:creatinine ratio and urine protein:creatinine ratio help differentiate underlying causes. Prompt identification and treatment of the underlying cause are critical to prevent irreversible damage. For a broader context, see our Renal Overview page.