Table of Contents
Overview – Malaria
Malaria is a life-threatening protozoan infection caused by Plasmodium species, transmitted by female Anopheles mosquitoes. It remains a major global health concern, particularly in tropical and subtropical regions, with Plasmodium falciparum responsible for the most severe and fatal cases. Clinical features range from cyclical fevers to severe multi-organ dysfunction, and diagnosis and treatment must be timely to prevent complications and mortality.
Definition
Malaria is a parasitic disease caused by infection with Plasmodium protozoa, transmitted through the bite of an infected female Anopheles mosquito. It causes recurrent fever, anaemia, and may lead to life-threatening complications.
Aetiology
- Pathogen: Plasmodium (eukaryotic protozoan)
- Species:
- P. falciparum – Most serious (not persistent in liver)
- P. vivax – Less serious, persistent in liver
- P. ovale – Less serious, persistent in liver
- P. malariae – Less serious, not persistent in liver
- P. knowlesi – Zoonotic, less common
Vector
- Anopheles mosquito
- Bites at night
- Breeds in shaded, vegetated, permanent water sources
Transmission Patterns
- Stable transmission: Continuous, endemic transmission
- Unstable transmission: Periodic epidemics, often following environmental changes
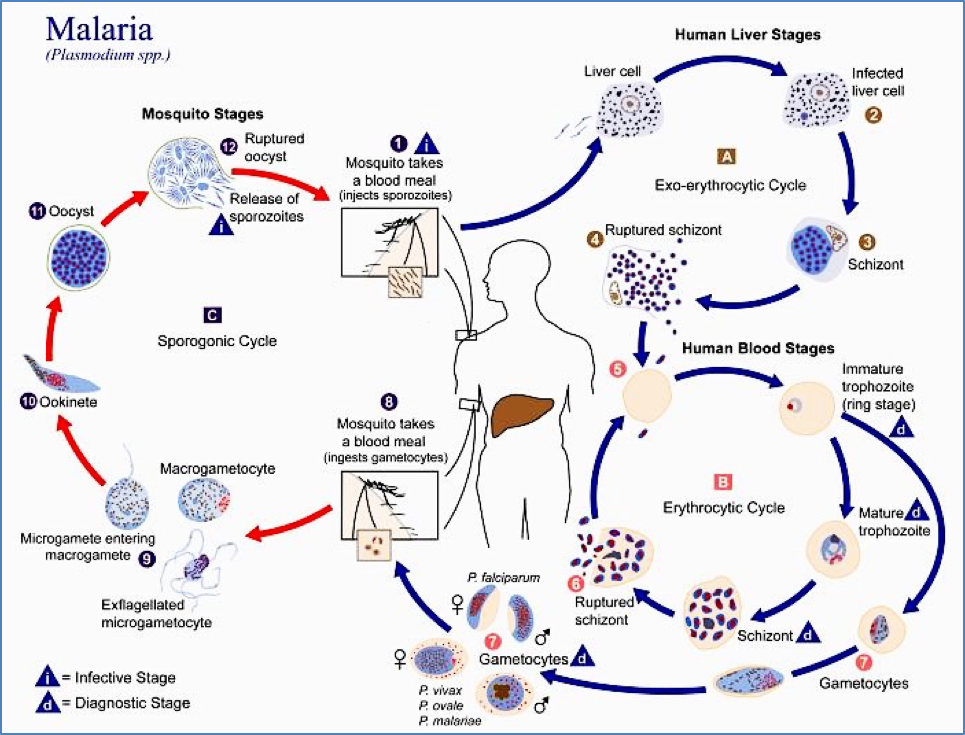
Lifecycle
- Mosquito bites infected human → ingests gametocytes
- Gametocytes → oocysts in mosquito gut → rupture → sporozoites
- Sporozoites migrate to mosquito’s salivary glands
- Sporozoites injected into new human host
- Sporozoites infect liver → multiply into merozoites
- Merozoites enter RBCs → cycle of replication and lysis
- Some merozoites become gametocytes → re-ingested by mosquitoes
Incubation Period
- Ranges from 2 weeks to several months depending on species and host immunity
Pathogenesis
- Red blood cell lysis → Pyrogens → cyclical fever
- Extravascular haemolysis (spleen) → Anaemia, haemoglobinuria
- Cytoadherence: RBCs become sticky → capillary blockage → hypoxia → multiorgan failure
- Cerebral malaria, pulmonary oedema, renal failure
- Immune complex deposition (Type III hypersensitivity) → arthritis, glomerulonephritis
Clinical Features
Uncomplicated Malaria (e.g. P. vivax, P. ovale):
- Episodic fever (tertian/quartan pattern)
- Headache, vomiting, diarrhoea
- Chills, sweating
- Muscle aches, dry cough
- Splenomegaly, jaundice
- May relapse due to liver hypnozoites
- Treatment: Primaquine (targets liver hypnozoites)
Complicated (Severe) Malaria – P. falciparum:
- Severe headache, nausea, vomiting
- Cerebral ischaemia, hallucinations, seizures, coma
- Severe anaemia (Hb 10–20 g/L), haemoglobinuria, renal failure
- Hepatosplenomegaly, hypoglycaemia, acidosis
- High fatality if untreated
- Treatment: Artemisinin derivatives (target blood-stage gametocytes)
Investigations
- Clinical suspicion: Endemic area + classic symptoms
- Microscopy: Thick and thin blood films (Giemsa stain)
- RDTs (Rapid Diagnostic Tests): Detect Plasmodium antigens
- PCR: High-sensitivity molecular diagnosis
Management
Gametocidal Agents
- Artemether/lumefantrine: First-line for P. falciparum
- Single-dose primaquine: Clears gametocytes
Hypnozoite-targeting Agents
- Primaquine: Prevents relapse in P. vivax and P. ovale infections
Supportive Care (for severe cases):
- Fluids and electrolytes
- Glucose monitoring (risk of hypoglycaemia)
- Management of seizures and coma
Prevention
- Chemoprophylaxis: For travellers (e.g. doxycycline, atovaquone-proguanil)
- Mosquito control: Nets, repellents, indoor residual spraying
- Environmental: Vector habitat reduction
- Vaccines: Some in development with partial protection
Immunity
- Acquired immunity: After repeated exposures (common in endemic areas)
- At-risk populations:
- Non-immunes (infants, travellers, pregnant women) → High severity risk
- Immunity is lost after extended absence from endemic zones
Genetic Protection
- Sickle cell trait: Infected cells rupture prematurely → less parasite replication
- Duffy antigen absence: Confers resistance to P. vivax
- G6PD deficiency, thalassemia: Partial protective effects
Summary – Malaria
Malaria is a protozoan parasitic disease caused by Plasmodium species and transmitted via Anopheles mosquitoes. It presents with episodic fevers and may progress to life-threatening complications, especially in P. falciparum infections. Management includes antimalarial agents such as artemisinin and primaquine, with prevention focused on vector control and prophylaxis. For a broader context, see our Microbiology & Public Health Overview page.