Table of Contents
Overview – Bowel Obstructions
Bowel obstructions are a common and potentially life-threatening cause of acute abdomen that can occur anywhere along the gastrointestinal tract. They may be mechanical or functional, partial or complete, and may involve the small or large intestine. Rapid recognition and differentiation between simple and strangulated bowel obstruction is essential, as delayed treatment in the latter can result in bowel necrosis, perforation, and death. This article outlines the causes, clinical features, investigations, and management of bowel obstruction—a key topic in surgical and emergency medicine rotations.
Definition
- Bowel obstruction refers to a blockage that prevents normal flow of intestinal contents.
- Can be classified as:
- Small bowel vs large bowel
- Mechanical (e.g., adhesions, hernias, volvulus) vs functional (e.g., paralytic ileus)
- Partial vs complete
- Strangulated vs non-strangulated
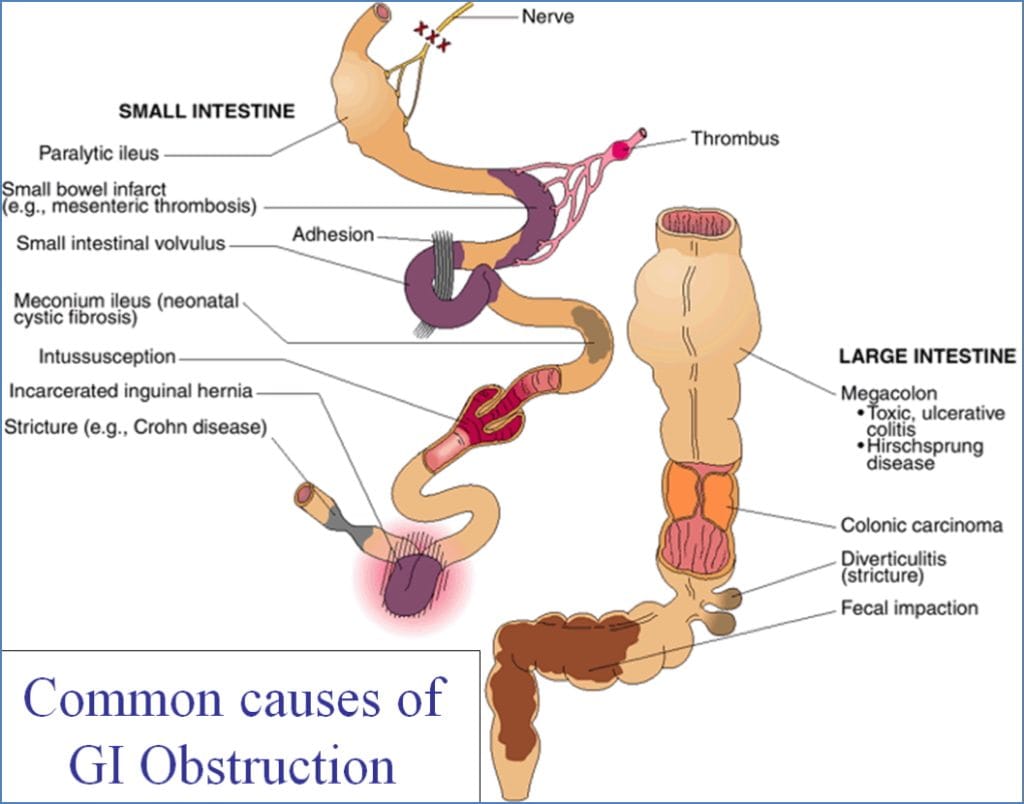
Causes of Bowel Obstruction
Small Bowel
- Adhesions (most common cause)
- Hernias (e.g., inguinal, femoral)
- Volvulus
- Intussusception
- Strictures (e.g., Crohn’s disease)
- Tumours
- Gallstone ileus
- Meconium ileus (in neonates)
Large Bowel
- Colorectal carcinoma
- Diverticulitis with stricture
- Fecal impaction
- Volvulus (sigmoid, caecal)
- Hirschsprung’s disease
- Toxic megacolon (e.g., UC)
Clinical Features
General Symptoms
- Abdominal distension
- Nausea and vomiting
- Cramping abdominal pain
- Obstipation (no flatus or stool)
By Obstruction Level
- Proximal (e.g., duodenum/jejunum):
→ Profuse, often bilious vomiting
→ Minimal distension - Mid-small bowel:
→ Moderate vomiting
→ Abdominal distension
→ Obstipation - Distal (e.g., colon):
→ Late-onset feculent vomiting
→ Marked distension
→ Complete obstipation
Features Suggesting Strangulation
- Shock (tachycardia, hypotension)
- Fever, leucocytosis
- Peritonism
- Vomiting of blood (gross or occult)
- Melena
- Bowel infarction risk
Investigations
Imaging
- Upright CXR: Look for free air under diaphragm (perforation)
- Abdo XR: Dilated loops of bowel, air-fluid levels
- CT Abdomen (Gold Standard): Identifies site, cause, and severity
- Ultrasound: Useful in pregnant patients or children

Laboratory
- Elevated WCC, lactate, and LDH (→ possible ischaemia)
- ↑ Amylase
- Electrolyte abnormalities
- Proximal SBO: → Metabolic alkalosis
- Infarction/strangulation: → Metabolic acidosis
- Signs of dehydration
Management
- Initial Resuscitation:
- IV fluids and electrolyte correction
- NG tube decompression
- Analgesia and antiemetics
- Urinary catheter to monitor output
- Surgical Referral for definitive management
- Conservative Management:
- Indicated for partial SBO
- Includes bowel rest, NG decompression, and observation
- Surgical Intervention:
- Indicated for complete obstruction or signs of strangulation
- May involve adhesiolysis, resection, or hernia repair
Complications
- Strangulation → ischaemia → necrosis → perforation
- Sepsis
- Peritonitis
- Hypovolaemia and shock
Prognosis
- Non-strangulating: ~2% mortality
- Strangulating: ~8% mortality (↑ to 25% if >36h)
- Strangulation with ischaemia/perforation: ~85% mortality
Summary – Bowel Obstructions
Bowel obstructions are a critical surgical emergency characterised by abdominal distension, vomiting, and constipation. Differentiating between small and large bowel, as well as between partial, complete, and strangulated obstruction, is essential for appropriate management. Early CT imaging and surgical referral are key to reducing morbidity and mortality. For more context, visit our Gastrointestinal Overview page.