Table of Contents
Overview – Addison’s Disease
Addison’s disease, also known as primary chronic adrenocortical insufficiency, is a rare endocrine disorder caused by the underproduction of adrenal hormones, most notably cortisol and aldosterone. This condition, most commonly due to autoimmune adrenalitis, results in profound fatigue, electrolyte imbalances, and, in severe cases, life-threatening Addisonian crisis. Understanding Addison’s disease is crucial for prompt diagnosis and management to prevent adrenal crisis and ensure hormonal replacement.
Definition
Addison’s disease is the primary failure of the adrenal cortex, leading to reduced secretion of glucocorticoids (cortisol), mineralocorticoids (aldosterone), and androgens. It is classified as a primary adrenal insufficiency.
Aetiology
Most Common Cause
- Autoimmune adrenalitis – responsible for ~70% of cases in developed countries.
Other Causes
- Tuberculosis (historically more common worldwide)
- Adrenal metastases
- Adrenal haemorrhage (e.g. Waterhouse-Friderichsen syndrome)
- Infiltrative diseases (e.g. amyloidosis, haemochromatosis)
- Congenital adrenal hyperplasia
- Iatrogenic causes (e.g. bilateral adrenalectomy)
Pathophysiology
- ↓ Cortisol → Impaired glucose metabolism, stress intolerance
- ↓ Aldosterone → Sodium loss, potassium retention → Hyponatraemia & Hyperkalaemia
- ↑ ACTH (due to feedback) → Stimulates melanocytes → Skin hyperpigmentation
Clinical Features
Early Non-Specific Symptoms
- Fatigue
- Weakness
- Lethargy
- Depression
Later Stage Symptoms
- Gastrointestinal:
- Anorexia
- Weight loss
- Vomiting, diarrhoea
- Skin:
- Hyperpigmentation (especially in sun-exposed areas, pressure points, palmar creases)
- Electrolyte Abnormalities:
- Hyponatraemia
- Hyperkalaemia
- Hypovolaemia (dizziness, hypotension)
Investigations
Initial Blood Tests
- UECs:
- ↓ Sodium
- ↑ Potassium
- ↑ Urea & Creatinine
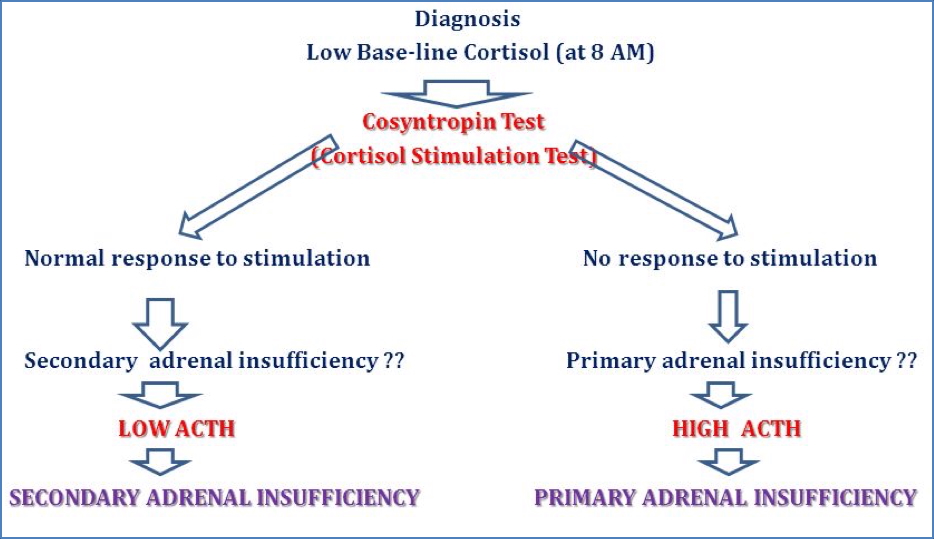
Diagnostic Testing
- Short Synacthen Test (Cortisol stimulation with synthetic ACTH)
- No increase in cortisol levels = Primary adrenal insufficiency
- Measure baseline and 30-minute post-injection cortisol/aldosterone
- Serology:
- Positive adrenal autoantibodies (Anti-21 hydroxylase)
- ACTH Levels:
- Elevated in primary Addison’s
- Differentiates from secondary adrenal insufficiency
Management
Hormonal Replacement
- Hydrocortisone – Glucocorticoid replacement
- Fludrocortisone – Mineralocorticoid replacement (if aldosterone is low)
Supportive
- Electrolyte correction
- Educate patients on stress-dose steroids (e.g. during illness or surgery)
Complications
Addisonian Crisis (Acute Adrenal Crisis)
Triggers
- Physical stress: infection, surgery, trauma
- Sudden withdrawal of corticosteroids
Clinical Features
- Severe hypotension and shock
- Abdominal pain
- Intractable vomiting
- Fever
- Confusion or coma
- Vascular collapse
Emergency Management
- IV fluids (normal saline ± dextrose)
- IV hydrocortisone
- Correction of electrolyte imbalances
- Treat underlying cause
Differential Diagnosis
- Secondary adrenal insufficiency (pituitary/hypothalamic dysfunction)
- Chronic fatigue syndrome
- Hypothyroidism
- Gastroenteritis
- SIADH (for hyponatraemia)
Summary – Addison’s Disease
Addison’s disease is a primary adrenal insufficiency marked by cortisol and aldosterone deficiency, often due to autoimmune adrenalitis. Patients present with non-specific symptoms like fatigue, hyperpigmentation, and characteristic electrolyte derangements. Diagnosis is confirmed with ACTH stimulation testing and managed with hormone replacement. Crisis prevention and education are vital. For further endocrine topics, see our Endocrine Overview.