Table of Contents
Overview – Upper Limb Neurological Examination
The upper limb neurological examination is a core OSCE skill used to localise lesions in the central or peripheral nervous system. It assesses motor, sensory, and reflex functions, as well as cerebellar coordination. This examination is critical for diagnosing pathologies such as stroke, brachial plexus injuries, motor neuron disease, and peripheral neuropathies. It involves a structured approach: inspection, tone, power, reflexes, coordination, and sensation — with attention to dermatomes and myotomes.
General Setup
- Wash hands, introduce yourself, confirm patient identity and age.
- Explain the examination and obtain consent.
- Patient seated at 45° or upright, with arms exposed (shirt off or sleeves rolled).
- Compare both sides throughout.
- Ask the patient to place the backs of their hands on their thighs.
- Observe surroundings for walking aids or medications (e.g., steroids, chemotherapy).
- Observe the patient for posture, speech, or signs of hemispatial neglect.
Inspection
- Wasting:
- Deltoid (axillary nerve injury)
- Thenar eminence (median nerve)
- Hypothenar eminence (ulnar nerve)
- Deformities: Erb’s palsy, Klumpke’s palsy, upper limb postures (e.g., decorticate, decerebrate).
- Fasciculations: Tap with reflex hammer to elicit (e.g., deltoid, biceps).
- Involuntary movements:
- Rest tremor: Parkinson’s disease
- Postural tremor: essential tremor, hyperthyroidism
- Intention tremor: cerebellar lesion
- Pronator drift test: indicates upper motor neuron (UMN) lesion if arm drifts and pronates.
Tone
- Test tone at shoulder, elbow, and wrist joints.
- Hypertonia (UMN lesions, Parkinsonism):
- Spasticity (velocity-dependent)
- Rigidity (lead-pipe or cogwheel)
- Hypotonia: Lower motor neuron (LMN) lesions, cerebellar disease
Power (Using MRC Grading 0–5)
Support joints while isolating muscles:
- Shoulder: Abduction – Axillary nerve (C5)
- Elbow: Flexion – Musculocutaneous (C5-C6); Extension – Radial (C7)
- Wrist: Extension – Radial (C7)
- Fingers:
- Flexion – Median and ulnar (C8)
- Extension – Radial (C7)
- Abduction – Ulnar (T1)
- Thumb: Abduction – Median (T1)
MRC grading:
- 0: No movement
- 1: Flicker
- 2: Movement without gravity
- 3: Against gravity
- 4: Against resistance
- 5: Normal
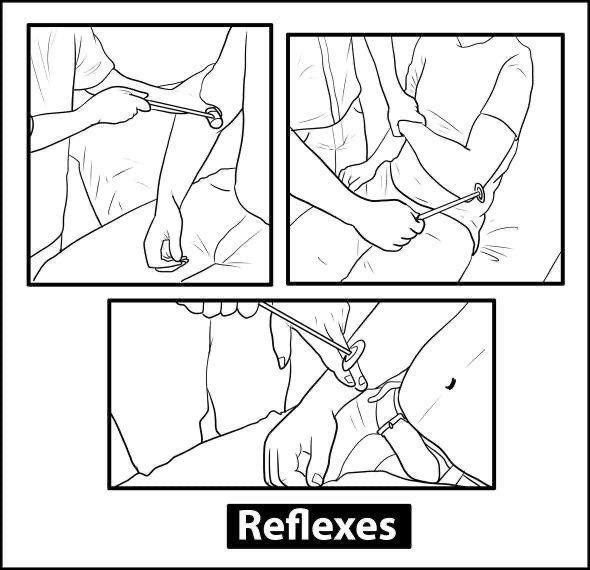
Reflexes
- Biceps (C5/C6)
- Brachioradialis (C5/C6)
- Triceps (C7)
Grading:
- 0: Absent
- 1: Present with reinforcement
- 2: Normal
- 3: Brisk
- 4: Clonus
Reinforcement manoeuvre: Ask patient to clench teeth.
Coordination
- Finger-to-nose test
- Past-pointing: suggests dysmetria
- Rapid alternating movements: dysdiadochokinesia in cerebellar disease

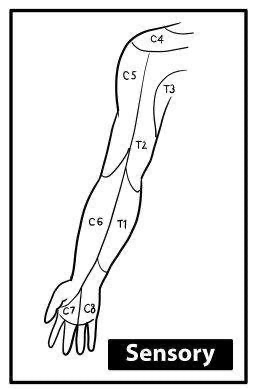
Sensation
Test with patient’s eyes closed, compare bilaterally.
- Light touch & pin-prick (dermatomes):
- C4: Shoulder
- C5: Lateral upper arm (“badge area”)
- C6: Thumb
- C7: Middle finger
- C8: Little finger
- T1: Medial forearm
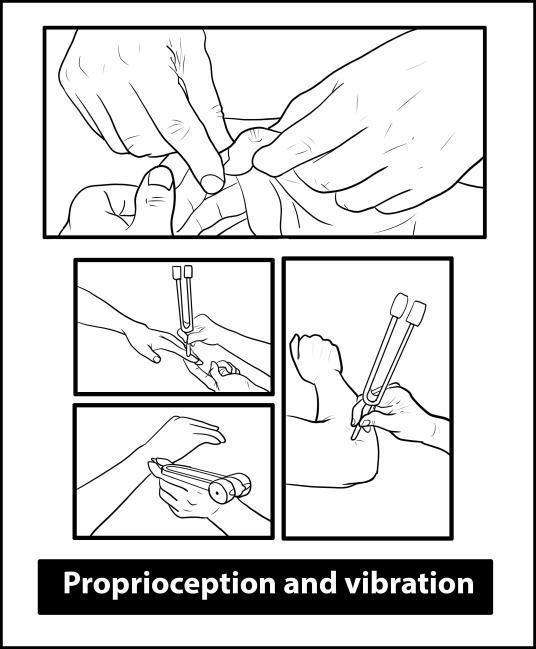
- Proprioception: Move distal phalanx up/down → progress proximally if impaired
- Vibration (128 Hz tuning fork): Start at index tip → radial styloid → olecranon
Special Tests
- Hoffmann’s reflex: Flick distal phalanx of middle finger → thumb flexion = UMN lesion above C5.
- Offer to examine lower limbs and cranial nerves if pathology suspected.
Localising Lesions
UMN vs LMN Features
| Feature | UMN | LMN |
|---|---|---|
| Tone | Hypertonia | Hypotonia |
| Reflexes | Hyperreflexia | Hyporeflexia |
| Fasciculations | Rare | Common |
| Muscle Wasting | Late (disuse) | Early |
| Babinski | Positive | Absent |
| Side | Contralateral (above decussation) | Ipsilateral |
Myotomes and Nerve Supply
| Muscle | Movement | Nerve | Root |
|---|---|---|---|
| Deltoid | Shoulder abduction | Axillary | C5 |
| Biceps | Elbow flexion | Musculocutaneous | C5–C6 |
| Triceps | Elbow extension | Radial | C7 |
| Extensor carpi | Wrist extension | Radial | C7 |
| Extensor digitorum | Finger extension | Radial | C7 |
| Flexor digitorum | Finger flexion | Median & Ulnar | C8 |
| Interossei | Finger abduction | Ulnar | T1 |
| Abductor pollicis brevis | Thumb abduction | Median | T1 |
Related Conditions
Brachial Plexus Injuries
- Erb-Duchenne Palsy (C5-C6): Waiter’s tip deformity, loss of shoulder abduction and elbow flexion.
- Klumpke’s Palsy (C8-T1): Total claw hand, affects intrinsic hand muscles, ± Horner syndrome.
Neurological Syndromes
- Syringomyelia: Cape-like sensory loss (pain/temp), LMN signs, Horner syndrome.
- Brown-Séquard Syndrome:
- Ipsilateral: motor, proprioception loss
- Contralateral: pain, temperature loss
Stroke Syndromes
- MCA: Contralateral face/arm weakness, aphasia (dominant), neglect (non-dominant)
- ACA: Contralateral leg weakness, personality change
- PICA: Wallenberg syndrome: cranial nerve deficits + Horner syndrome
Summary – Upper Limb Neurological Examination
The upper limb neurological examination is a structured assessment to localise central and peripheral neurological lesions. It includes inspection, tone, power, reflexes, coordination, and sensation, and is vital for diagnosing stroke, nerve injuries, and neuromuscular disorders. For a broader context, see our Clinical Skills Overview page.