Table of Contents
Overview – Spinal Cord Syndromes
Spinal cord syndromes refer to distinct clinical patterns resulting from injury or ischemia to specific regions of the spinal cord. Recognising these patterns—such as Brown-Séquard syndrome, anterior cord syndrome, central cord syndrome, and dorsal column syndrome—is critical in neurology and emergency medicine. Final-year medical students must be able to identify which spinal tracts are affected and correlate them with sensory or motor deficits. This page outlines the key features, affected tracts, and clinical consequences of each syndrome.
Definition
Spinal cord syndromes are neurologic disorders resulting from focal lesions to the spinal cord, leading to predictable patterns of sensory and motor deficits depending on the tracts involved.
Aetiology
- Trauma (e.g. stab wounds, motor vehicle accidents, diving injuries)
- Ischemia (e.g. anterior spinal artery infarction)
- Tumours or spinal stenosis
- Inflammatory or infectious myelitis
Spinal Cord Tract Refresher
- Dorsal Column – Medial Lemniscal pathway: Discriminative touch & proprioception (ipsilateral)
- Lateral Corticospinal Tract: Voluntary motor control (ipsilateral)
- Spinothalamic Tract: Pain, temperature, crude touch (contralateral)
Clinical Features
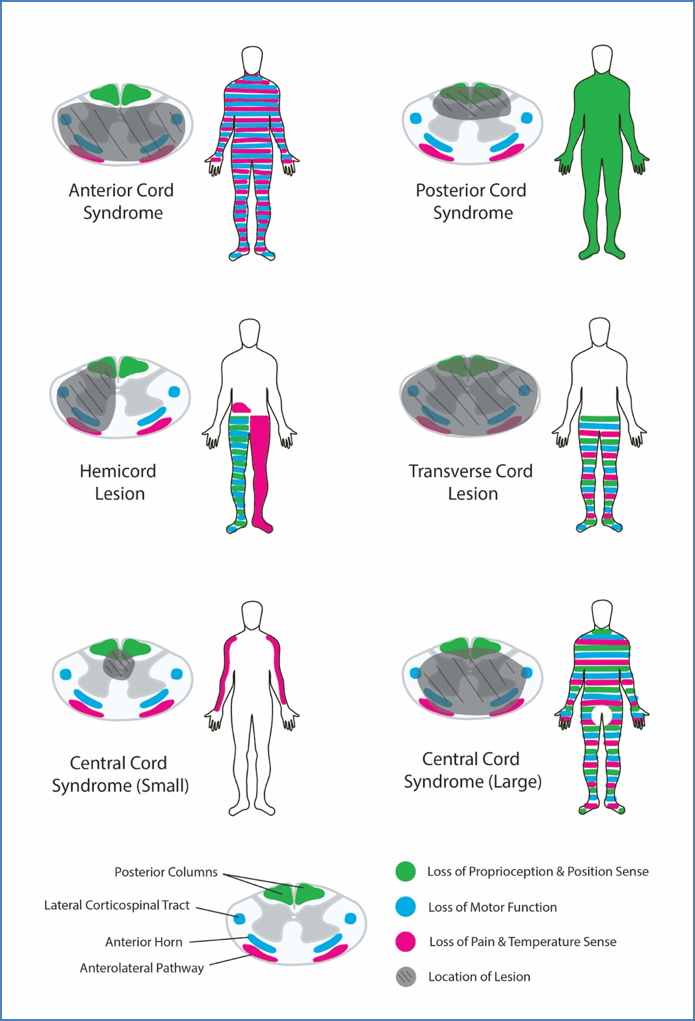
Brown-Séquard Syndrome (Hemicord Lesion)
Classically caused by penetrating trauma (e.g. stab wound)
- Ipsilateral below the lesion:
- Loss of proprioception & vibration (dorsal columns)
- Loss of voluntary motor function (corticospinal tract)
- Contralateral below the lesion:
- Loss of pain & temperature sensation (spinothalamic tract)
Anterior Cord Syndrome (Anterior Spinal Artery Infarction)
Often caused by trauma (e.g. hyperflexion injury or diving)
- Motor loss below lesion: Corticospinal tract affected → bilateral paralysis
- Pain & temperature loss below lesion: Spinothalamic tract affected
- Vibration & proprioception spared: Dorsal column preserved
- Possible autonomic dysfunction: Hypotension, urinary retention, sexual dysfunction
Central Cord Syndrome
Most common in elderly with cervical spondylosis after trauma
- Upper limb motor impairment > lower limb impairment (corticospinal tract centrally located)
- Variable sensory loss below the lesion
- Disproportionate upper limb weakness
Dorsal Column Syndrome
Rare; often secondary to Vitamin B12 deficiency or neurosyphilis
- Ipsilateral loss of proprioception & vibration below lesion (dorsal columns)
- Pain, temperature & motor function preserved
Investigations
- MRI spine – gold standard for anatomical localisation and aetiology
- CT spine – useful in trauma
- Bloods – look for B12, syphilis, autoimmune markers
- Lumbar puncture – if infection or inflammation suspected
Management
- Initial Stabilisation:
- Spinal immobilisation in trauma
- High-dose steroids if indicated (controversial)
- Definitive Treatment:
- Surgical decompression (e.g. tumour, abscess, disc herniation)
- Treat underlying cause (e.g. antibiotics for infection, revascularisation for ischemia)
- Neurorehabilitation and supportive care
Complications
- Permanent motor/sensory deficits
- Autonomic dysfunction
- Neurogenic bladder and bowel
- Pressure sores from immobility
- Spasticity and contractures
Differential Diagnosis
- Multiple sclerosis
- Transverse myelitis
- Epidural abscess or hematoma
- Peripheral neuropathies
- Stroke (especially brainstem infarcts)
Summary – Spinal Cord Syndromes
Spinal cord syndromes present with characteristic patterns of neurological deficit depending on the tracts involved. Recognising conditions like Brown-Séquard syndrome, anterior cord syndrome, central cord syndrome, and dorsal column syndrome is crucial in both diagnosis and early management. These syndromes demand prompt localisation and appropriate investigation to avoid long-term disability. For a broader context, see our Nervous System Overview page.