Table of Contents
Overview – The Neurological Examination
The neurological examination is a cornerstone of clinical medicine, providing essential information on the integrity of the central and peripheral nervous systems. A thorough neurological examination assesses cranial nerves, motor and sensory pathways, cerebellar function, and gait, helping to localise lesions and identify life-threatening pathology such as raised intracranial pressure, stroke, or spinal cord compromise.
Cranial Nerve Examination
General Inspection
- Alertness and orientation (person, place, time)
- Level of consciousness
- Facial asymmetry or trauma
- Muscle wasting, fasciculations, tremors
- Speech abnormalities (dysphasia, dysarthria, dysphonia)
- Ptosis or inability to close the eyes
- Facial muscle wasting or sweating
CN I – Olfactory
- Ask: “Have you noticed any change in smell or taste?”
CN II – Optic
- Ask about recent vision changes
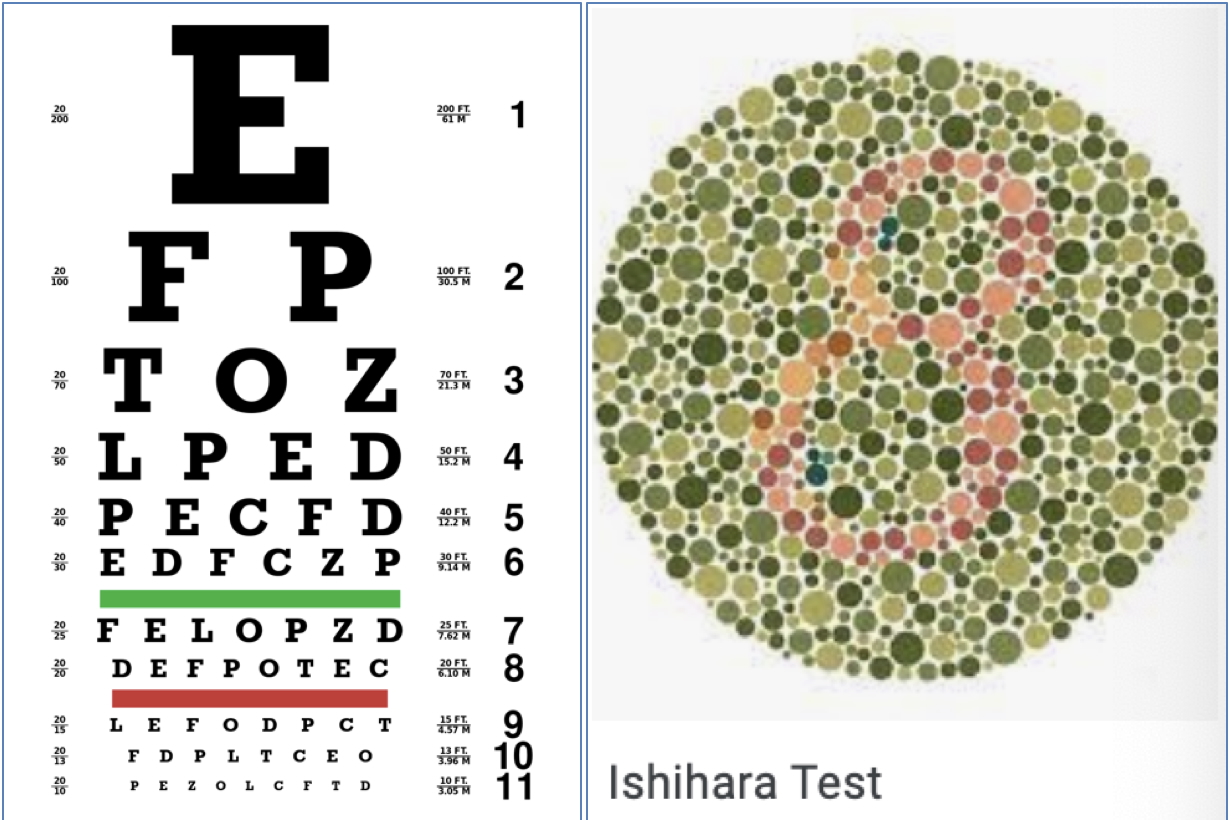
- Visual acuity (Snellen chart; test each eye separately, then both)
- Colour vision (Ishihara plates)
- Visual field testing (confrontation method using hat pin)
- Pupil reactions (direct, consensual, and swinging light test)
- Fundoscopy for signs of:
- Cataracts
- Diabetic or hypertensive retinopathy

CN III, IV, VI – Oculomotor, Trochlear, Abducens
- “Follow the hat pin with your eyes – keep your head still”
- Ask: “Do you see double at any point?”
- Perform 6-position gaze test
- Observe for:
- Asymmetric eye movement
- Nystagmus (indicates cerebellar lesion – points to lesion side)
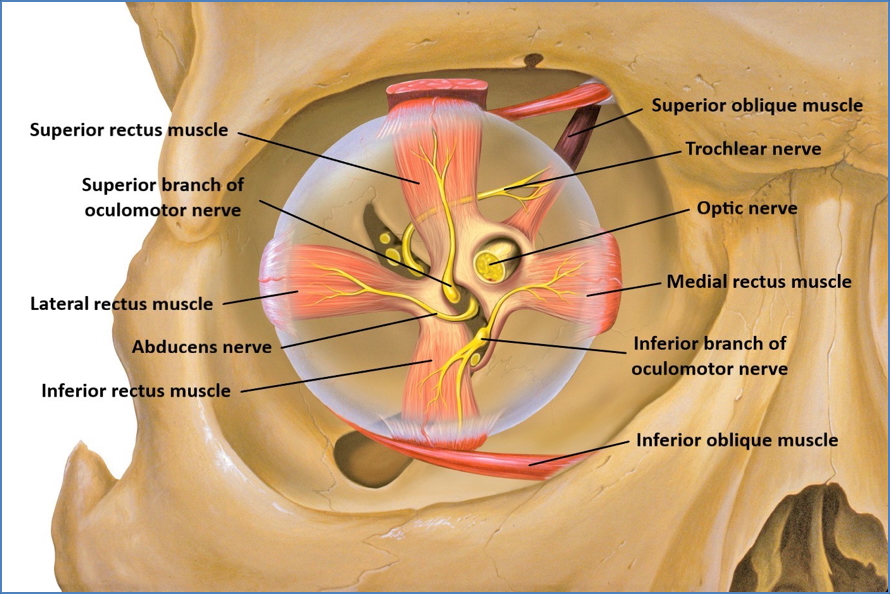
CN III: Superior/Inferior/Medial rectus + Inferior oblique
CN IV: Superior oblique
CN VI: Lateral rectus
CN V – Trigeminal
Sensory:
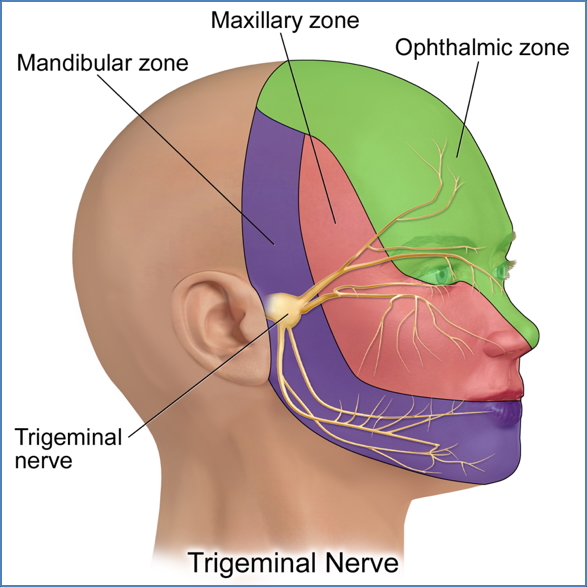
- Sharp/pain (demonstrate on sternum) → Ophthalmic, Maxillary, Mandibular branches
- Light touch (cotton wool) → Same three branches
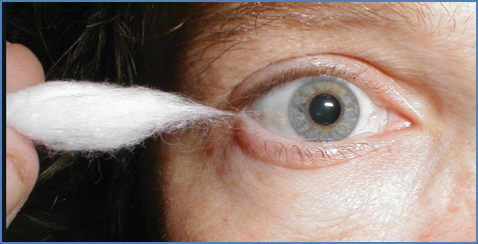
- Corneal reflex (rolled cotton from the side)
Motor:
- Clench jaw → Masseter
- Open jaw against resistance → Pterygoids
- Jaw jerk reflex (tap with mouth relaxed)
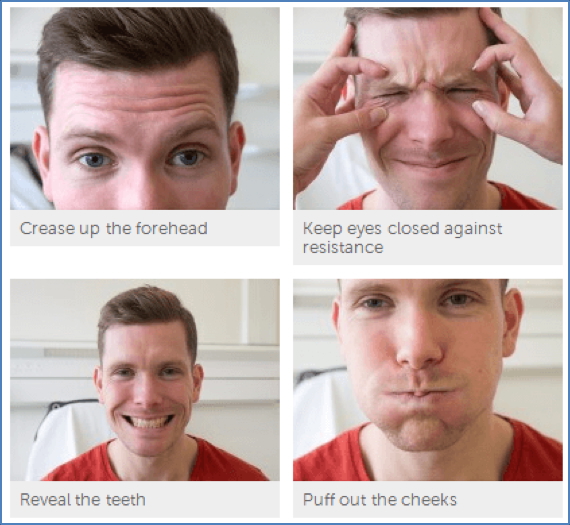
CN VII – Facial
- Wrinkle forehead (frontalis)
- Close eyes tightly (orbicularis oculi)
- Smile (zygomaticus)
- Puff cheeks (buccinator)
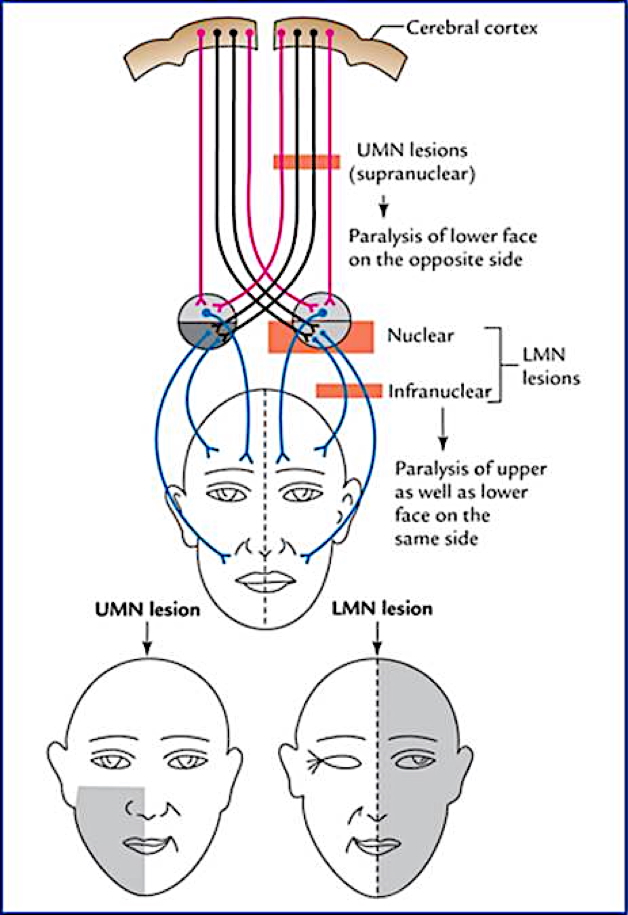
UMN: Lower face weakness (contralateral)
LMN: Entire half face weakness (ipsilateral)
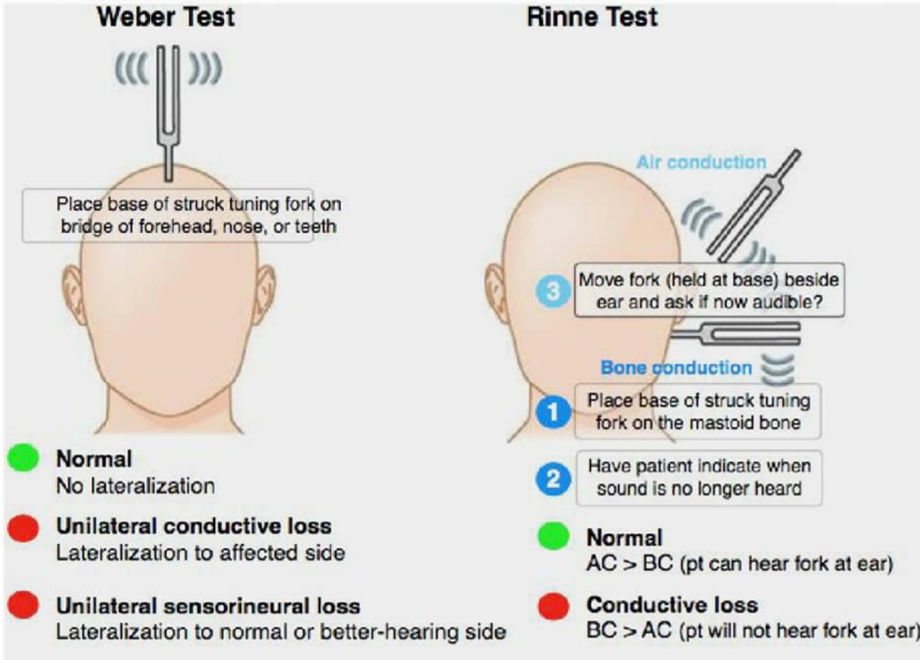
CN VIII – Vestibulocochlear
- Hearing: Whisper test (distract opposite ear)
- Tuning fork tests:
- Weber: Lateralisation indicates conductive loss on that side
- Rinne: Air vs bone conduction
- Romberg’s Test (close eyes, feet together)
CN IX & X – Glossopharyngeal & Vagus
- Say “Ah” → Observe uvula elevation (asymmetry = vagus lesion)
- Gag reflex (mention only)
- Say name (hoarseness = vagus involvement)
- Cough (bovine cough = vocal cord paralysis)
CN XI – Accessory
- Turn head against resistance (sternocleidomastoid)
- Shrug shoulders against resistance (trapezius)

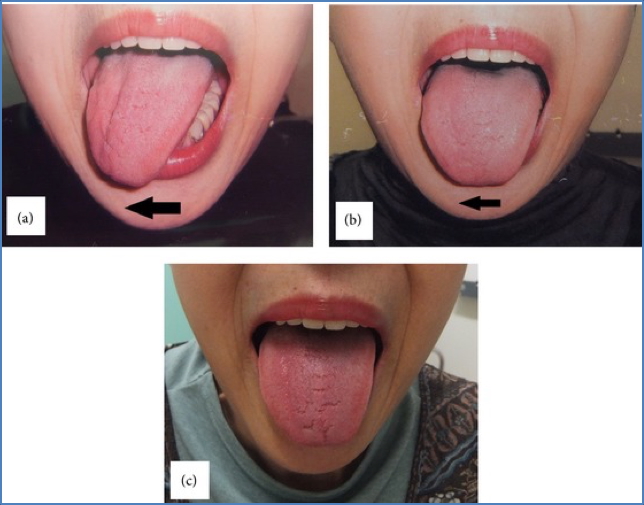
CN XII – Hypoglossal
- Stick tongue out
- Deviation = lesion on same side
Cerebellar Examination
General Inspection
- Alertness
- Tremors, fasciculations, wasting
- Head injury signs
Coordination and Function
- Speech: “British Constitution” (dysarthria/dysphasia)
- Eye Movements: Horizontal nystagmus
- Romberg’s Test:
- Falls with eyes closed = proprioceptive
- Falls with eyes open = cerebellar
- Gait: Normal, heel-to-toe, wide-based?
- Pronator Drift: Upward = cerebellar; downward = pyramidal
- Rebound Test
- Dysdiadochokinesis: Rapid alternating movements
- Finger-nose test: Past pointing = cerebellar

Supine Testing
- Heel-shin test
- Toe-finger test
- Clonus: Rhythmic contraction on rapid dorsiflexion
- Truncal ataxia: Arms crossed, standing from sitting without hands

Upper Limb Neurological Examination
General Inspection
- Shirt off, hands visible
- Note: Muscle wasting, fasciculations, scars, bruising, asymmetry
Motor
- Tone (passive movement):
- Shoulder, elbow, wrist, fingers
- Hypertonia = UMN; Hypotonia = LMN
- Power (grade 0–5):
- Shoulder: Abduction (C5-C6), Adduction (C7-C8)
- Elbow: Flexion (C5-C6), Extension (C7-C8)
- Wrist: Flexion/Extension (C6–C8)
- Fingers: Grip, abduction, adduction, thumb opposition (C7–T1)
Reflexes
- Biceps (C5-C6)
- Triceps (C6-C7)
- Brachioradialis (C5-C6)
Coordination
- Pronator drift
- Rebound test
- Dysdiadochokinesis
- Finger-nose test
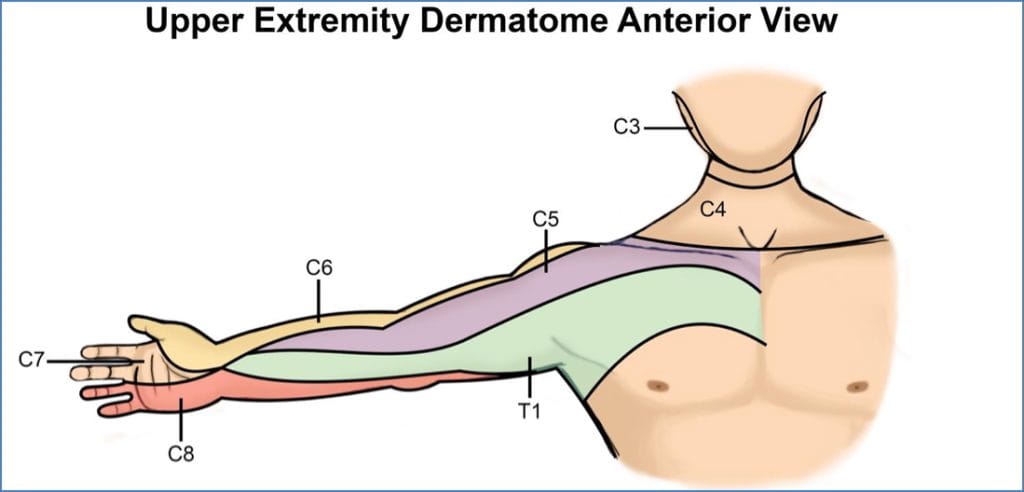
Sensory
Test over C3–T2 dermatomes:
- Pain (spinothalamic)
- Light touch (both pathways)
- Vibration & proprioception (dorsal column)
- Always demonstrate on sternum first
Lower Limb Neurological Examination
General Inspection
- Standing: Wasting, fasciculations, involuntary movements, deformities
Gait
- Walk normally
- Look for: Foot drop (L4–L5), shuffling (Parkinson’s), wide-based (cerebellar)
- Heel-toe walking
- Romberg’s Test
Motor (on couch)
- Tone: Hip, knee, ankle, toes
- Power:
- Hip: Flexion/Extension/Abduction/Adduction (L2–S2)
- Knee: Flexion (L5–S1), Extension (L3–L4)
- Ankle: Dorsi (L4–L5), Plantarflexion (S1)
Reflexes
- Patellar (L3–L4)
- Achilles (S1)
- Plantar response (Babinski)
Coordination
- Heel-shin test
- Toe-finger test
- Dysdiadochokinesis
- Clonus
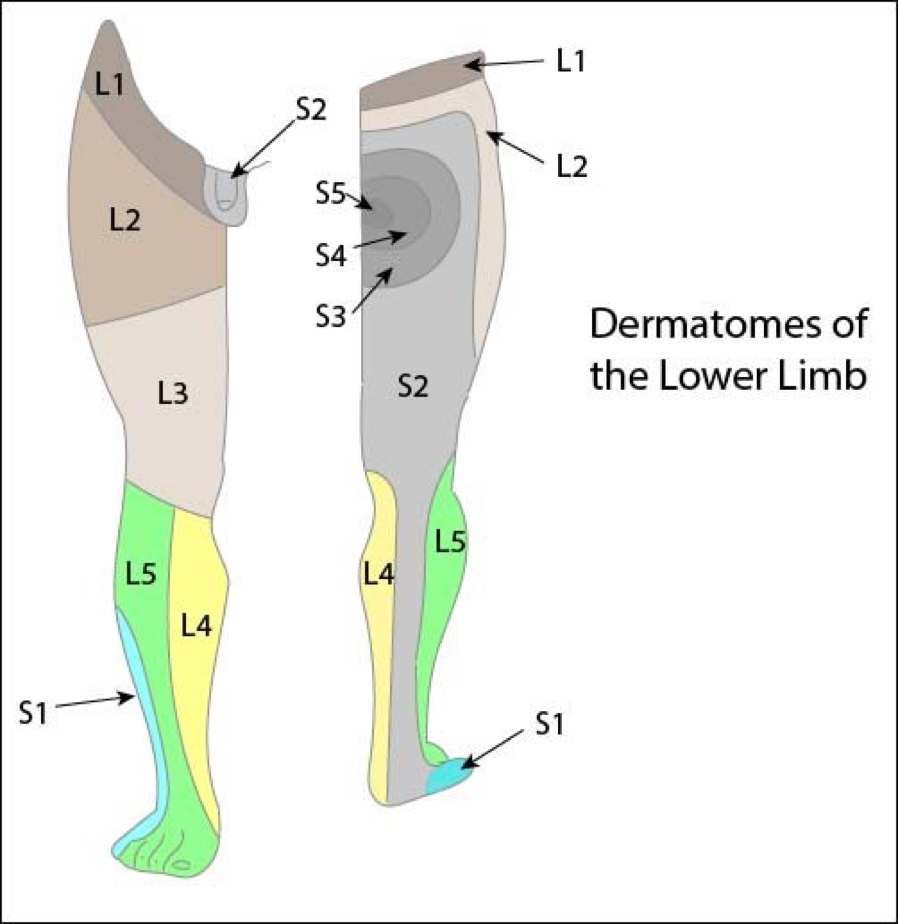
Sensory
Test dermatomes L1–S2:
- Pain, vibration, proprioception, light touch (eyes closed)
Special Tests (Meningitis)
- Kernig’s Sign: Pain on hip flexion and knee extension
- Brudzinski’s Sign: Involuntary leg flexion with neck flexion
- Neck Stiffness: Pain on flexion
Summary – The Neurological Examination
The neurological examination is an indispensable clinical tool for assessing cranial nerves, motor and sensory function, and cerebellar integrity. It allows for lesion localisation, identification of central and peripheral nervous system dysfunction, and detection of urgent red flag signs. For a broader context, see our Clinical Skills Overview page.