Table of Contents
Overview – The Ageing Heart
The ageing heart undergoes predictable structural, histological, and functional changes that affect cardiovascular performance, especially under stress. Although many of these changes are considered normal (termed “normal ageing myopathy”), they reduce cardiac reserve and increase vulnerability to heart failure. Understanding these adaptations is vital for recognising age-related cardiac limitations and distinguishing them from pathological conditions.
What Happens in a Normal Ageing Heart?
Structural Changes
- Heart dilation: enlarged lumen of left atrium and left ventricle
- Valve calcification, especially mitral → slows closure and prolongs filling
- Increased capillary density
- Increased myocardial fibrosis
- Less compliant arteries
Histological Changes
- ↓ Number of myocytes
- Compensatory hypertrophy of remaining myocytes
- Thickened heart walls due to increased stress from stiffer arteries
Functional & Metabolic Changes
- ↓ Heart rate during exercise
- ↓ Contractility due to:
- Reduced mitochondrial metabolism
- Impaired sarcoplasmic reticulum calcium handling (↓ Ca²⁺ storage and pumps)
Autonomic Sensitivity Changes
- ↓ β-adrenergic sensitivity → ↓ maximum heart rate and contractility
- ↓ Baroreceptor and chemoreceptor sensitivity
Electrical Conduction Changes
- Fibrotic, calcified conduction pathways
- ↓ Sinoatrial node pacemaker cells → reduced resting heart rate
- Impaired sinoatrial node function → predisposition to arrhythmias and atrial fibrillation
Clinical Significance
Normal Ageing Myopathy
- The above changes are physiological and not inherently pathological
- However, they decrease the heart’s functional reserve, particularly during exercise
Risk Factor for Heart Failure
- Age-related cardiac changes interact with each other or coexisting disease to cause failure
- Examples:
- Myocyte loss + valve calcification → ↓ stroke volume
- Fibrosis + stiff arteries + valvular stenosis → ↑ afterload
- Atherosclerosis + ↓ contractility → ↓ coronary perfusion → ischaemia
- Hypertension + stiffened arteries → impaired ventricular ejection
Functional Comparison by Age
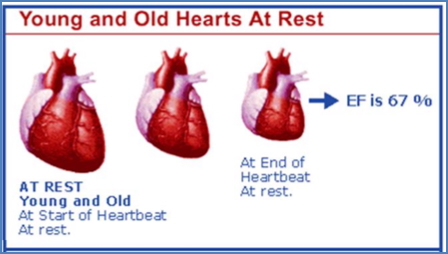
At Rest – 20yo vs 80yo
- Heart Rate: 10% ↓ in elderly
- Stroke Volume: 10% ↑ in elderly
- Cardiac Output: Unchanged (↓ HR × ↑ SV)
- Ejection Fraction: Maintained (≈67%)
During Exercise
- ↑ Preload in older adults (via longer filling time and ventricular dilation)
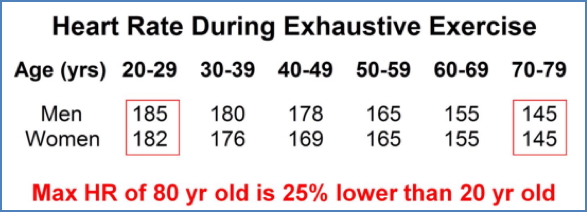
- ↓ Max heart rate → ↓ overall cardiac output (by ~25%)
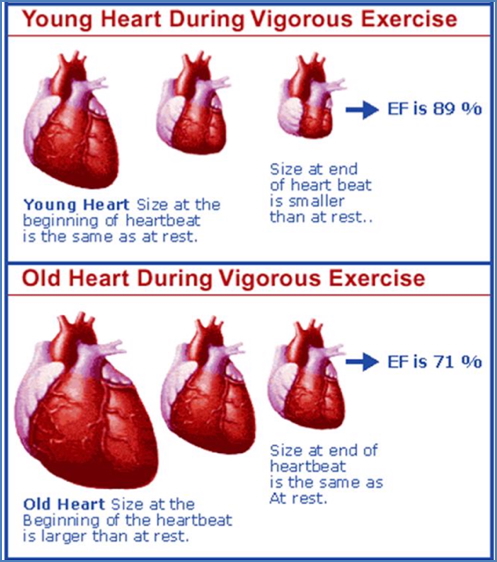
- ↓ Max ejection fraction (young: up to 89%, old: only 71%)
- ↓ VO₂max due to:
- ↓ muscle mass
- ↓ mitochondrial efficiency
- ↓ enzyme activity

Compensation Strategy
- Young Heart: Boosts contractility → ↓ end-systolic volume → ↑ stroke volume
- Old Heart: Compensates by ↑ preload (dilation) → ↑ end-diastolic volume → ↑ stroke volume
- However, excessive dilation → ↑ left atrial pressure → pulmonary congestion (mimicking heart failure)
Management
Lifestyle
- Aerobic exercise improves many aspects of cardiac ageing:
- ↑ contractility
- ↑ ejection fraction
- ↑ oxygen consumption
- ↓ arterial stiffness
- ↓ need for excessive dilation
Pharmacological Interventions
- Agents that:
- ↑ vascular compliance
- ↓ cardiac fibrosis
- ↓ ventricular hypertrophy
- Antioxidants (reduce oxidative damage)
- Anti-inflammatory drugs (target underlying inflammation)
Summary – The Ageing Heart
The ageing heart exhibits reduced contractility, impaired conduction, and stiffened vasculature, all of which limit cardiovascular performance under stress. These changes, while considered normal, increase the risk of heart failure especially when interacting with comorbid conditions. For a broader context, see our Cardiovascular Overview page.