Table of Contents
Overview – Carcinoid Heart Disease
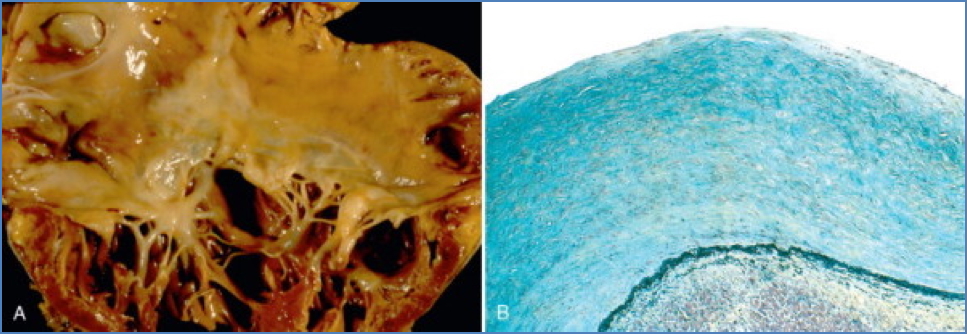
Carcinoid heart disease is a rare but significant complication of carcinoid syndrome, resulting from serotonin-secreting neuroendocrine tumours. These tumours release vasoactive substances that travel through the bloodstream to the right side of the heart, leading to endocardial and valvular fibrosis. If unrecognised, this condition can lead to progressive right heart failure. It is an important differential in any patient with unexplained right-sided valvular disease and systemic symptoms such as flushing or diarrhoea.
Definition
Carcinoid heart disease is a cardiac manifestation of carcinoid syndrome, characterised by fibrotic degeneration of the right-sided heart valves—primarily the tricuspid and pulmonary valves—due to circulating vasoactive amines from carcinoid tumours.
Aetiology
- Occurs secondary to carcinoid syndrome, caused by neuroendocrine tumours (usually in the GI tract or lungs)
- Tumours secrete serotonin, bradykinin, histamine, and prostaglandins into the venous system
Pathophysiology
- Vasoactive substances released into systemic venous circulation
- These drain into the right side of the heart, where they cause:
- Endocardial fibrosis
- Thickening and retraction of valve leaflets, particularly:
- Tricuspid valve → Tricuspid regurgitation
- Pulmonary valve → Pulmonary regurgitation
- Left heart involvement is rare (as hormones are metabolised in the lungs)
Clinical Features
Systemic (Carcinoid Syndrome)
- Episodic facial flushing
- Abdominal cramps
- Nausea, vomiting, diarrhoea
Cardiac
- Tricuspid Regurgitation (most common)
- Hepatomegaly and right upper quadrant pain
- Pulsatile liver
- Raised JVP with prominent v-waves
- Systolic murmur @ 4th ICS, left sternal edge, ↑ with inspiration
- Pulmonary Regurgitation
- Dyspnoea
- Diastolic murmur @ 2nd ICS, left sternal edge, ↑ with inspiration
- Signs of Right Heart Failure
- Peripheral oedema
- Ascites and organomegaly
- Raised JVP
- Signs of portal hypertension: caput medusae, spider naevi
Investigations
- 24-hour urinary 5-HIAA (serotonin metabolite) – diagnostic
- Abdominal CT or MRI – to identify primary tumour
- Somatostatin receptor scintigraphy (SRS) – tumour localisation
- Echocardiography – assess valvular involvement and cardiac function
- ECG and CXR – supportive but non-specific findings
Management
Medical
- Somatostatin analogues (e.g. octreotide) – inhibit hormone secretion
- Interferon-α – for palliation in advanced disease
Surgical
- Tumour resection – where feasible
- Valvular surgery (e.g. valvuloplasty or valve replacement) – if symptomatic right heart failure
Complications
- Progressive right heart failure
- Hepatic metastases
- Portal hypertension
- Reduced survival without tumour control
Prognosis
- Early detection and resection of the primary tumour improve outcomes
- Cardiac involvement signifies advanced disease, often requiring multimodal treatment
Differential Diagnosis
- Primary tricuspid or pulmonary valve disease
- Infective endocarditis
- Ebstein anomaly (if tricuspid involvement)
- Right-sided heart failure of other causes (e.g. pulmonary hypertension, COPD)
Summary – Carcinoid Heart Disease
Carcinoid heart disease is a serious complication of carcinoid syndrome, primarily affecting the right side of the heart due to exposure to serotonin and other vasoactive substances. It typically presents with tricuspid and pulmonary valve regurgitation, leading to right heart failure. Early recognition, biochemical testing (urinary 5-HIAA), and tumour localisation are essential. Treatment involves somatostatin analogues, surgical tumour resection, and valve repair if required. For broader context, see our Cardiovascular Overview page.