Table of Contents
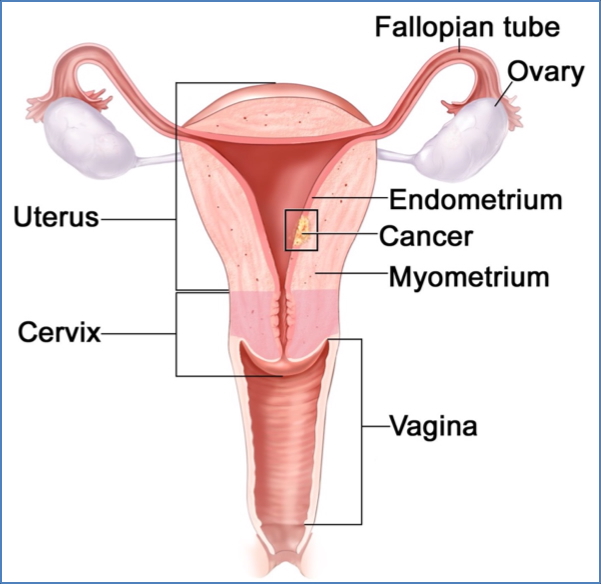
Overview – Uterine Cancers
Uterine cancers are among the most common gynaecological malignancies, with endometrial adenocarcinoma being the predominant subtype, especially in postmenopausal women. Less common, but more aggressive, is uterine leiomyosarcoma, a rare tumour of the uterine smooth muscle. Early recognition of symptoms—particularly abnormal bleeding—can significantly improve survival outcomes.
Endometrial Adenocarcinoma
Aetiology
- Excessive oestrogen exposure is the key risk factor
- Risk factors include:
- Early menarche, nulliparity, late menopause
- Obesity, polycystic ovarian syndrome (PCOS)
- Prolonged unopposed oestrogen therapy (including hormone replacement therapy, tamoxifen use)
- Hypertension, diabetes, pelvic radiation
- May progress from endometrial hyperplasia
Pathogenesis
- Oestrogen excess + genetic predisposition → Endometrial hyperplasia → Dysplastic transformation → Adenocarcinoma
Morphology
Macroscopic
- Polypoid/cauliflower-like masses
- Uterine enlargement
- Necrotic or haemorrhagic areas
Microscopic
- Back-to-back crowded endometrial glands
- Dysplastic cells with minimal intervening stroma
- Features of malignancy: nuclear atypia, mitotic figures
Clinical Features
- Epidemiology: Most common gynaecological cancer, typically in women >60 years
- Symptoms:
- Postmenopausal or intermenstrual bleeding
- Lower abdominal pain or cramping
- Anaemia
- Thin, watery, or clear vaginal discharge
Investigations
- Endometrial biopsy via Pipelle aspiration or curettage
- Transvaginal ultrasound: Endometrial thickness >5mm is suspicious
- Hysteroscopy: For exclusion of fibroids, hyperplasia or polyps
Management
- Staging: Chest X-ray, CT, MRI, PET scan
- Baseline tumour marker: CA-125
- Surgical:
- Total hysterectomy
- Bilateral salpingo-oophorectomy
- Pelvic lymphadenectomy
- ± Adjuvant radiotherapy or chemotherapy (based on staging)
Prognosis
- High early detection rate due to bleeding → 90% 5-year survival
- Advanced disease has poor outlook → ~15% 5-year survival
Uterine Leiomyosarcoma
Aetiology
- Unknown; likely a mix of genetic and environmental factors
Pathogenesis
- Malignant tumour of uterine smooth muscle (myometrium)
- NOT hormonally driven
- May occur in other smooth muscle locations (e.g. stomach, small intestine, retroperitoneum)
Morphology
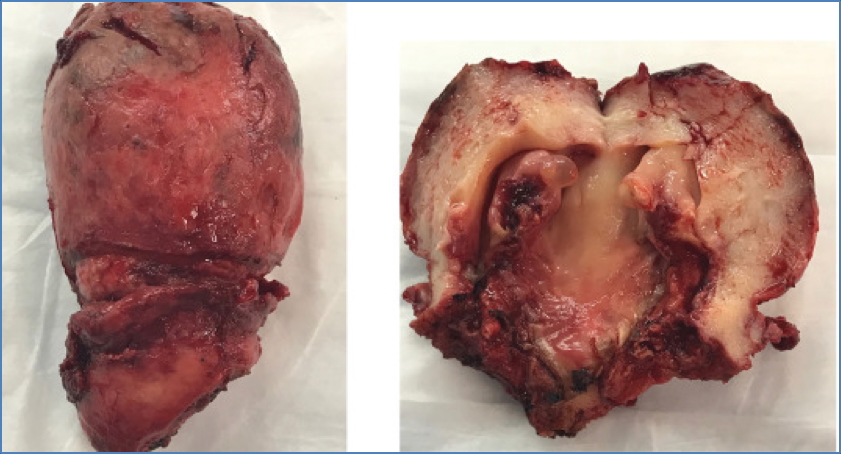
Macroscopic
- Large (>10 cm), soft, fleshy mass
- Yellow-tan colour
- Poorly demarcated, no capsule
- Often shows haemorrhage and necrosis
Clinical Features
- Rare: Accounts for ~1% of uterine cancers
- Age: Usually 40–60 years
- Presents late, often with metastatic or advanced disease
- Symptoms:
- Abnormal bleeding (often dysfunctional)
- Pelvic or abdominal pain
- Systemic signs: weight loss, fatigue, fever
- Enlarged uterus; may prolapse into vagina
Diagnosis
- Definitive diagnosis requires hysteroscopic biopsy
- Imaging is not sufficient alone
Management
- Total hysterectomy is standard
- ± Radiation and/or chemotherapy
Prognosis
- Poor prognosis due to aggressive spread
- <70% 5-year survival, often much lower in advanced stages
Summary – Uterine Cancers
Uterine cancers include both common endometrial adenocarcinoma and rare, aggressive leiomyosarcoma. While adenocarcinoma often presents early with postmenopausal bleeding and has high survival rates, leiomyosarcoma presents late and carries a much worse prognosis. Timely biopsy and imaging are key to accurate diagnosis. For more, visit our Reproductive Health Overview page.