Table of Contents
Overview – Eating Disorders
Eating disorders are serious mental health conditions characterised by persistent disturbances in eating behaviour that significantly impair physical health or psychosocial functioning. Common types include anorexia nervosa and bulimia nervosa, each with distinct clinical profiles and risks. Eating disorders often emerge in adolescence or early adulthood and can be life-threatening without appropriate intervention. Understanding the psychological, social, and biological contributors is crucial for early detection and effective management.
Definition
- A persistent disturbance in eating behaviour that negatively affects physical health or psychosocial functioning.
- Often associated with distorted body image, fear of weight gain, and maladaptive coping strategies.
Aetiology
Eating disorders have a multifactorial origin, including:
- Individual Factors:
- Perfectionism
- Sense of lacking control
- History of sexual abuse
- Personality Factors:
- Obsessive-compulsive traits
- Histrionic and borderline personality features
- Family Environment:
- Dysfunctional family dynamics
- Emphasis on control and weight regulation
- Cultural/Societal Factors:
- Common in industrialised societies
- Media idealisation of thinness
Risk Factors
- Physical:
- Obesity
- Chronic illnesses (e.g. diabetes)
- Psychological:
- Career pressures to remain thin (e.g. athletes, dancers)
- Family history of mood disorders, substance use, or eating disorders
- Co-existing psychiatric disorders:
- Depression
- Obsessive-compulsive disorder (OCD)
- Anxiety disorders (especially panic disorder, agoraphobia)
- Substance use (especially linked with bulimia nervosa)
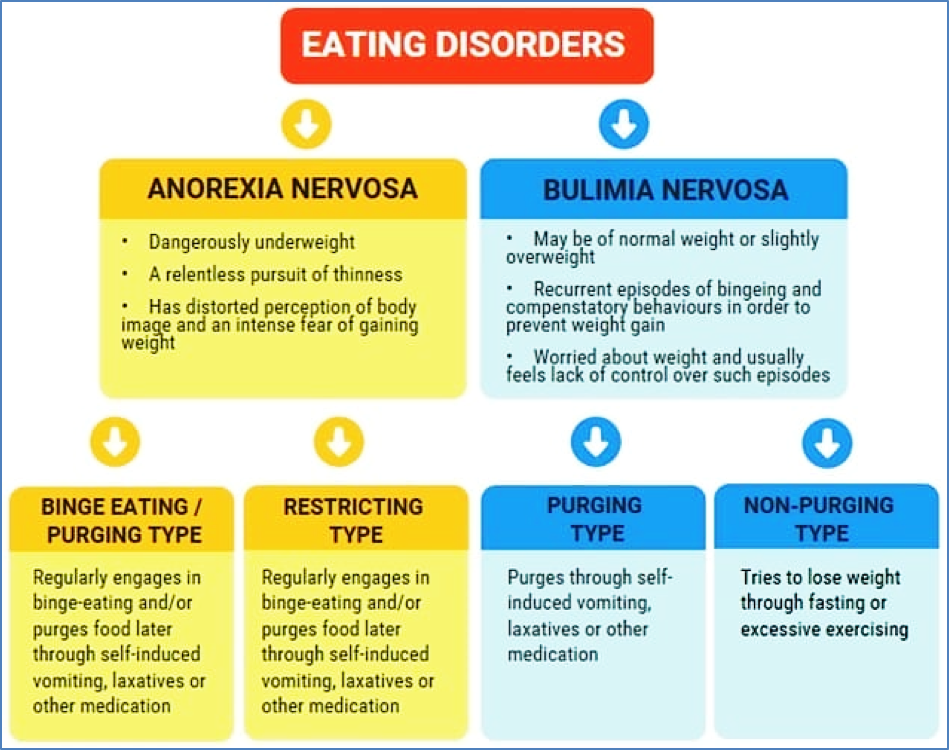
Anorexia Nervosa
DSM-5 Diagnostic Criteria
A. Restriction of energy intake → significantly low body weight
B. Intense fear of gaining weight or persistent behaviour interfering with weight gain
C. Body image disturbance or denial of the seriousness of low body weight
- Specifiers (based on BMI):
- Mild: BMI ≥17 kg/m²
- Moderate: BMI 16–16.99
- Severe: BMI 15–15.99
- Extreme: BMI <15
Management
- Psychotherapy is the gold standard:
- Individual, group, or family-based
- Focuses on body perception, coping strategies, and health education
- Outpatient programs are common
- Hospitalisation is rarely required unless medically indicated
Prognosis
- Early treatment leads to better outcomes
- Adolescents respond more favourably than adults
- 70% achieve ≥85% expected weight with treatment
- Long-term mortality 10–20%, often due to medical complications or suicide
Bulimia Nervosa
DSM-5 Diagnostic Criteria
A. Recurrent binge-eating episodes characterised by:
- Excessive food intake in a discrete period
- Sense of loss of control during the episode
B. Compensatory behaviours: vomiting, laxatives, diuretics, fasting, or excessive exercise
C. Behaviour occurs ≥1x/week for ≥3 months
D. Body image distortion influences self-evaluation
E. Not exclusive to anorexia nervosa episodes
- Specifiers (based on frequency of compensatory behaviours):
- Mild: 1–3/week
- Moderate: 4–7/week
- Severe: 8–13/week
- Extreme: 14+/week
Clinical Features
- Fatigue, muscle weakness
- Electrolyte imbalances
- Dental erosion
- Oedema
- Russell’s Sign: calluses on knuckles from vomiting
Management
- Medical:
- Manage electrolyte disturbances
- SSRIs (e.g. fluoxetine)
- Psychological:
- Cognitive behavioural therapy (CBT)
- Family therapy
- Psychoeducation
- Social:
- Normalise eating routines
- Address dysfunctional body image beliefs
Prognosis
- High relapse rate
- Adolescents often recover within 2 years
- Late-onset cases have poorer outcomes
Summary – Eating Disorders
Eating disorders are complex psychiatric conditions marked by disordered eating behaviours, distorted body image, and significant health consequences. Early recognition, multidisciplinary management, and targeted psychotherapy improve prognosis. For a broader context, see our Psychiatry & Mental Health Overview page.