Table of Contents
Overview – Analgesics
Analgesics are drugs that relieve pain by acting on the peripheral or central nervous system. They range from mild non-steroidal anti-inflammatory drugs (NSAIDs) to potent opioids and are used in acute, chronic, and neuropathic pain management. Matching the analgesic to the severity and nature of the pain is essential to ensure effective treatment while minimising side effects and the risk of dependency. This article outlines analgesic drug classes, mechanisms, and principles of rational pain management.
Principles of Pain Management
1. Evaluate the Pain
- Assess pain scale, nature of injury, history, and patient context (e.g. culture, mental health).
- Evidence suggests that if analgesics are properly matched to pain severity, addiction risk is minimal.
2. Match the Analgesic to the Pain
- Use the WHO Analgesic Ladder as a guide.
- Don’t undertreat severe pain (e.g. morphine for severe trauma, not aspirin).
3. Start Low, Titrate Up
- Adjust for individual variability in analgesic response.
- Avoid overdose and ensure adequate relief.
4. Monitor and Reassess
- Taper opioids when pain improves (e.g. post-operative pain).
- Chronic/neuropathic pain may require long-term management without step-down.
Clinical Reminder: Inadequate pain management is considered unethical and unacceptable.
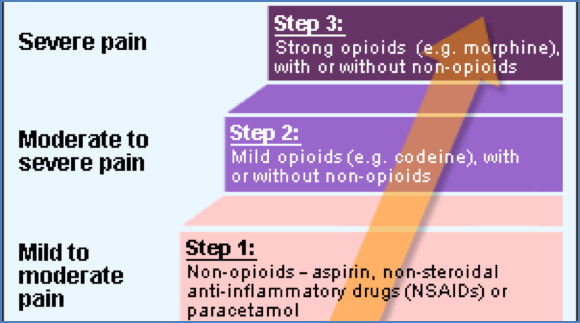
WHO Analgesic Ladder
- Developed for cancer pain, but applies to all pain.
- Start at the level matching the patient’s pain severity:
- Step 1: Mild pain → NSAIDs/Paracetamol
- Step 2: Moderate pain → Weak opioids ± NSAIDs
- Step 3: Severe pain → Strong opioids ± NSAIDs
NSAIDs & Related Drugs
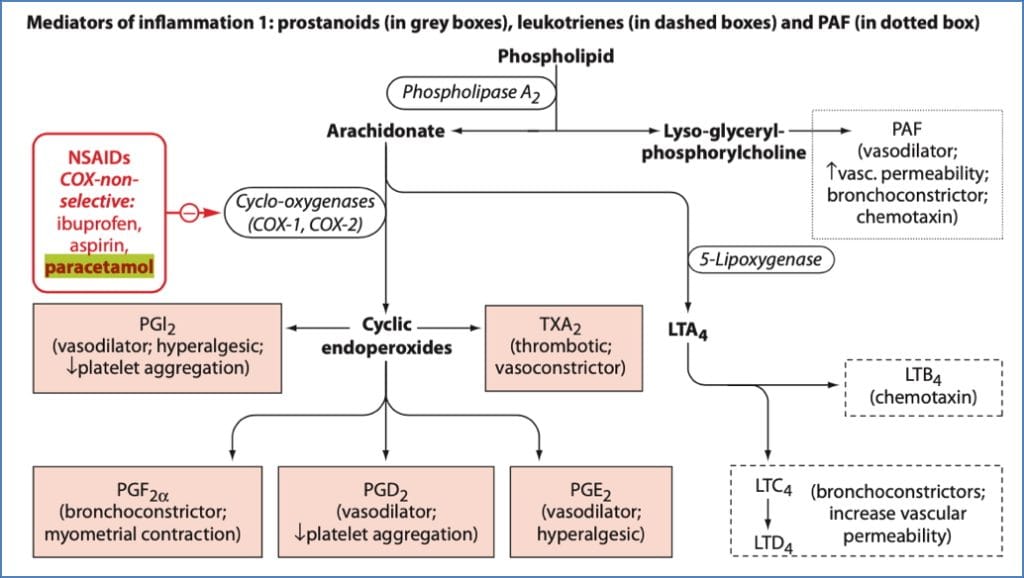
NSAIDs (e.g. Aspirin, Ibuprofen)
- MOA: Inhibit COX → ↓ prostaglandin production
- Effect: Reduces inflammation and prostaglandin-induced nociceptor hypersensitivity
- Also inhibits bradykinin effects
Paracetamol
- MOA: Poorly understood; possibly central COX-3 inhibition
- Effect: Analgesic and antipyretic (minimal anti-inflammatory)
- Often used synergistically with opioids
COX-2 Inhibitors (e.g. Celecoxib)
- MOA: Selective COX-2 inhibition → fewer GI side effects
- Effect: Anti-inflammatory and analgesic
Opioids
Classification & Mechanism
- Opiates: Derived from opium poppy
- Opioids: Includes synthetic analogues
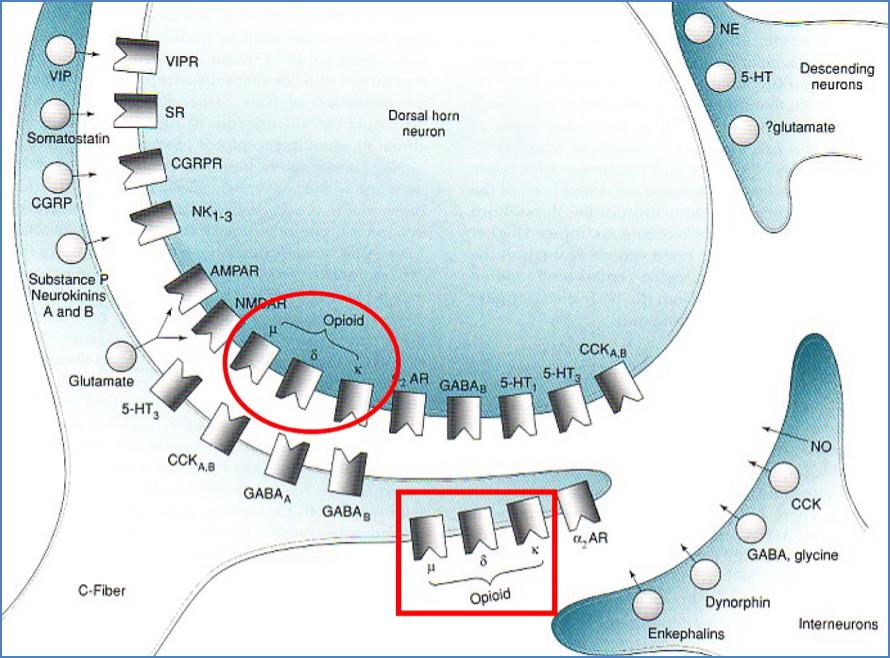
- Receptors: µ, δ, κ — all G-protein coupled
- Actions:
- Pre-synaptic: ↓ Ca²⁺ influx → ↓ neurotransmitter release
- Post-synaptic: Opens K⁺ channels → hyperpolarisation

Opioid Drug Summary
| Drug | Indications | Key Details |
|---|---|---|
| Codeine | Mild–moderate | Pro-drug converted to morphine; risk of constipation, respiratory depression |
| Tramadol | Mild–moderate | Weak µ-agonist + inhibits NA/5HT reuptake; risk of serotonin syndrome, seizures |
| Pethidine | Moderate–severe | Short-term use; toxic metabolite (norpethidine) may cause seizures |
| Morphine | Moderate–severe | Standard µ-agonist; versatile routes of administration |
| Hydromorphone | Severe pain | ~8x morphine potency; used in opioid-tolerant patients |
| Oxycodone | Moderate–severe | Oral bioavailability superior to morphine; high abuse potential |
| Fentanyl | Severe pain | 80x morphine potency; rapid onset, risk of muscle rigidity |
Opioid Side Effects & Monitoring
Common Side Effects:
- Respiratory depression
- Constipation
- Sedation, mood changes
- Histamine release (itch, urticaria)
- Urinary retention
- Tolerance (dose escalation)
Monitor:
- Respiratory rate, SpO₂
- BP, HR
- Mental status
- Bowel/bladder function
Antidote:
- Naloxone (Narcan): Competitive opioid receptor antagonist
- Rapidly reverses respiratory depression
- May cause return of pain
Atypical Analgesics
Used in chronic or neuropathic pain, or when opioids/NSAIDs are ineffective.
Tricyclic Antidepressants (TCAs)
- MOA: Inhibit reuptake of noradrenaline & serotonin → strengthens descending pain inhibition
- Additional benefits: Mood, sleep, and anxiety improvements
- Use: 1st line in neuropathic pain
Antiarrhythmics (e.g. Lignocaine, Mexiletine)
- MOA: Block VG-Na⁺ channels → ↓ ectopic firing
- Use: Residual neuropathic pain
Anticonvulsants
- Carbamazepine: Na⁺ channel blocker → used in trigeminal neuralgia, sharp/electric pain
- Gabapentin: GABA analogue → enhances inhibition in CNS; used in nerve injury and diabetic neuropathy
Neuropathic Pain Management
Stepwise Approach:
- 1st line: TCAs
- Residual pain: Add antiarrhythmics or anticonvulsants
- Last resort:
- Intrathecal opioids
- Spinal cord stimulation
- Deep brain stimulation
- Neurosurgery
Serotonin Syndrome – A Serious Risk
Triggered by serotonergic agents (e.g. TCAs, MAO inhibitors, tramadol)
Symptoms:
- Cognitive:
- Agitation, delirium, coma
- CNS Signs:
- Hyperthermia, tachycardia, mydriasis
- GI Signs:
- Nausea, diarrhoea
- Motor Signs:
- Tremor, clonus, ataxia
- Blood Changes:
- Leukocytosis, ↑ muscle enzymes, DIC

Summary – Analgesics
Analgesics include NSAIDs, paracetamol, opioids, and atypical agents used to manage acute, chronic, and neuropathic pain. Rational prescribing requires matching the drug to the pain type and severity, titrating doses carefully, and monitoring for side effects. The WHO Analgesic Ladder is a useful framework, and adjunct therapies like TCAs and anticonvulsants expand treatment options for complex pain. For a broader context, see our Pharmacology & Toxicology Overview page.