Table of Contents
Overview – Motor Neurone Disease
Motor neurone disease (MND), also known as amyotrophic lateral sclerosis (ALS), is a rapidly progressive neurodegenerative disorder that affects both upper and lower motor neurons. It leads to muscle weakness, atrophy, fasciculations, and spasticity, while sparing sensory and cognitive functions in most patients. Recognising the combined presence of UMN and LMN signs is key to early diagnosis. This page outlines the core pathology, clinical features, and prognosis of motor neurone disease.
Definition
Motor neurone disease (MND) is a degenerative condition of both upper and lower motor neurons, leading to progressive muscle weakness and wasting without sensory impairment. ALS is the most common subtype.
Aetiology
- 90% Sporadic
- 10% Genetic (e.g. SOD1, C9orf72 mutations)
Pathophysiology
- Degeneration of:
- Lower motor neurons (LMNs) in the anterior horn and cranial nerve nuclei
- Upper motor neurons (UMNs) in corticospinal tracts
- Results in:
- Loss of voluntary muscle control
- Progressive denervation and muscle wasting
- Sensory system is spared

Morphology
Macroscopic
- Atrophy of ventral horns of spinal cord
- Degeneration of ventral spinal roots
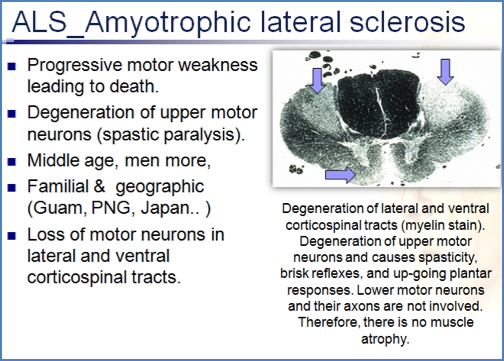
- Loss of lateral and ventral corticospinal tracts
Microscopic
- Neuronal degeneration with:
- Skein-like inclusions
- Bunina bodies
- Astrogliosis
- Spongiosis

Clinical Features
- Onset: Typically >40 years; rapid progression
- LMN signs:
- Progressive muscle weakness (distal → proximal)
- Amyotrophy (muscle wasting)
- Fasciculations and cramps
- Hyporeflexia (when LMN dominant)
- UMN signs:
- Spasticity, stiffness
- Hyperreflexia (due to loss of cortical inhibition)
- Upgoing plantar reflex (Babinski sign)
- Additional:
- Bulbar symptoms: Dysarthria, dysphagia
- Respiratory failure (late stage)
- No sensory, visual, or bladder involvement
Investigations
- Clinical diagnosis – based on combined UMN + LMN signs
- EMG/Nerve conduction studies – denervation pattern
- MRI – to exclude other causes (e.g. cervical myelopathy)
- Genetic testing – in suspected familial cases
Management
- Supportive care:
- Non-invasive ventilation (e.g. BiPAP)
- Nutritional support (PEG feeding if needed)
- Physiotherapy, speech therapy, palliative input
- Medications:
- Riluzole (glutamate antagonist) – modest survival benefit
Complications
- Respiratory failure
- Aspiration pneumonia
- Malnutrition and dehydration
- Depression and anxiety
- Progressive disability and dependence
Prognosis
- Incurable
- Median survival: 2–3 years from diagnosis
- Most deaths due to respiratory complications
Differential Diagnosis
- Cervical spondylotic myelopathy
- Multiple sclerosis
- Myasthenia gravis
- Kennedy’s disease
- Inclusion body myositis
Summary – Motor Neurone Disease
Motor neurone disease (MND) is a rapidly progressive and fatal condition characterised by degeneration of both upper and lower motor neurons. It presents with a mix of spasticity, muscle wasting, fasciculations, and areflexia, while sparing sensation. Supportive care is essential, and diagnosis is clinical. For a broader context, see our Nervous System Overview page.