Table of Contents
Overview – Neurovascular Compromise
Neurovascular compromise occurs when trauma causes damage to the nerves and blood vessels near bones and joints. It is a surgical emergency that can result in ischaemia, paralysis, or limb loss if not recognised and managed promptly. This guide covers key fracture-dislocation patterns that commonly injure neurovascular structures, associated functional deficits, and how to assess patients for compromise.
Definition
Neurovascular compromise is a condition in which nerve and/or vessel integrity is disrupted, often due to trauma. This leads to:
- Sensory or motor loss (neurological compromise)
- Impaired blood flow or bleeding (vascular compromise)
- Risk of permanent dysfunction or tissue necrosis if untreated
Common Injuries Causing Neurovascular Compromise
Upper Limb Fractures
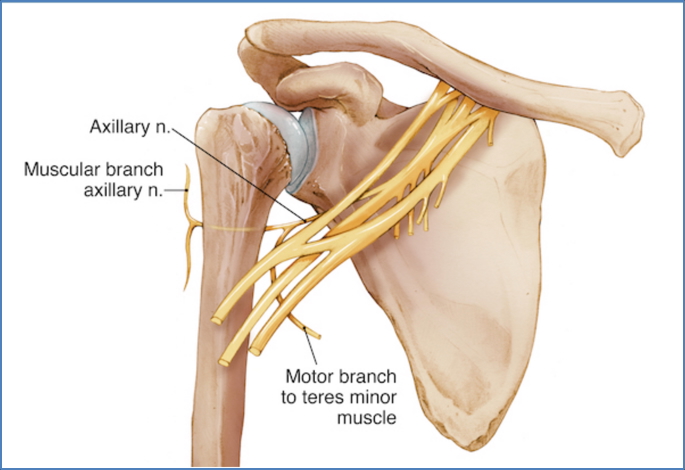
- Humeral Neck Fracture → Axillary nerve
- Mid-shaft Humerus → Radial nerve (via radial groove)
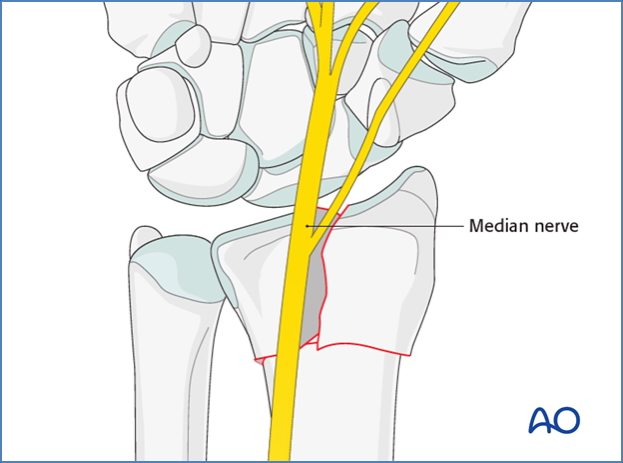
- Supracondylar Humerus Fracture → Median nerve and brachial artery

- Distal Radius (Colles’) Fracture → Median nerve, Ulnar nerve, Radial artery
- Combined Radius & Ulna Wrist Fracture → Median and Ulnar nerves, Radial and Ulnar arteries

Lower Limb Fractures
- Femoral Shaft Fracture → Femoral nerve, Sciatic nerve, Femoral artery

- Neck of Femur Fracture → Sciatic nerve, Femoral nerve, Femoral artery
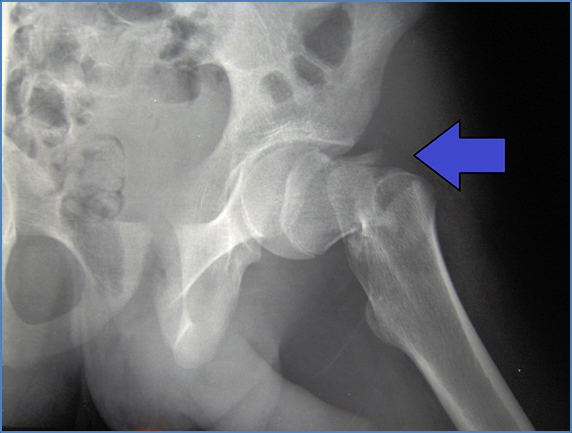

2. https://www.msdmanuals.com/home/multimedia/figure/fx_repairing_hip
- Ankle Fracture → Tibial nerve, Posterior tibial artery

Dislocations and Nerve Injury Risks
- Shoulder Dislocation (Glenohumeral):
- Axillary nerve
- Musculocutaneous nerve
- Radial nerve
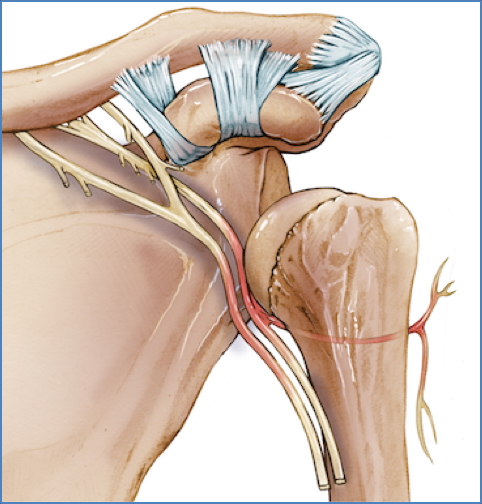
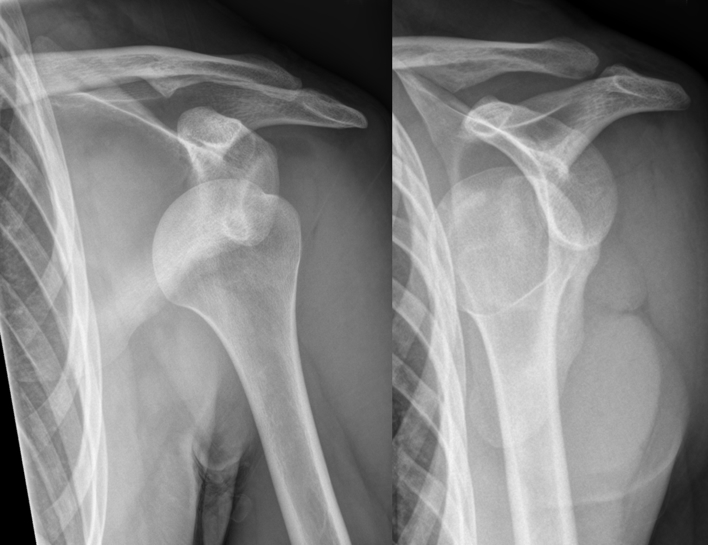
3. Hellerhoff, CC BY-SA 3.0 <https://creativecommons.org/licenses/by-sa/3.0>, via Wikimedia Commons
- Hip Dislocation:
- Sciatic nerve

- Knee Dislocation:
- Tibial nerve
- Common fibular nerve
- Popliteal artery and vein

- Ankle Dislocation:
- Tibial nerve
- Posterior tibial artery

Laceration Risk Zones
- Volar (Palmar) Wrist Laceration — Often seen in penetrating trauma (e.g. suicide attempts)
- Median nerve
- Ulnar nerve
- Radial and ulnar arteries
- Basilic and cephalic veins
- Wrist flexor tendons
Functional Deficits by Nerve
Upper Limb Nerve Injury Patterns
| Nerve | Typical Injury Site | Motor Loss | Sensory Loss |
|---|---|---|---|
| Axillary | Shoulder dislocation | Loss of shoulder abduction (deltoid) | Skin over deltoid region |
| Musculocutaneous | Axilla | Weak elbow flexion | Lateral forearm |
| Radial (Axilla) | Axilla | Wrist drop; ↓ elbow extension | Posterior arm, forearm, hand dorsum |
| Radial (Elbow) | Cubital fossa | Weak supination & wrist extension | Variable loss over dorsum |
| Median (Elbow) | Elbow region | Weak wrist/finger flexion; ↓ thumb opposition | Lateral 3.5 fingers palmar |
| Median (Wrist) | Wrist laceration | Thenar wasting; ↓ thumb opposition | Same as above |
| Ulnar (Above elbow) | Elbow fracture | Weak wrist/finger flexion (medial digits) | Medial 1.5 fingers |
| Ulnar (Wrist) | Wrist laceration | Claw hand (lumbrical dysfunction) | Medial 1.5 fingers |
Lower Limb Nerve Injury Patterns
| Nerve | Typical Injury Site | Motor Loss | Sensory Loss |
|---|---|---|---|
| Femoral | Femoral neck or shaft | ↓ Knee extension, hip flexion | Anterior thigh, medial lower leg |
| Obturator | Hip dislocation/fracture | ↓ Hip adduction | Medial thigh |
| Sciatic | Hip or femoral fracture | ↓ Knee flexion, foot/toe movement | Posterior leg & foot |
| Tibial | Tibial fracture/laceration | ↓ Plantarflexion, toe flexion | Sole of foot |
| Common Fibular | Fibular head injury | Foot drop; ↓ toe extension, ankle eversion | Lateral leg, dorsum of foot |
How to Test for Neurovascular Compromise
Vascular Assessment
- Bleeding or expanding haematoma → Suggests arterial injury
- Absent distal pulses → High suspicion for vessel injury
- Present distal pulses → Less likely but not ruled out
Neurological Assessment
- Sensory loss or tingling → Possible nerve injury
- Motor deficit (e.g. drop foot or wrist drop) → Likely nerve damage
- Normal function → Monitor, but early signs may be subtle
Summary – Neurovascular Compromise
Neurovascular compromise can result from fractures, dislocations, or lacerations that damage nearby nerves or blood vessels. Clinical suspicion should be high in high-risk injury patterns, especially around joints. Early detection via thorough motor, sensory, and vascular examination is essential to prevent irreversible damage or limb loss. For broader context, see our Musculoskeletal Overview page.