Table of Contents
Overview – Haemophilia A & B
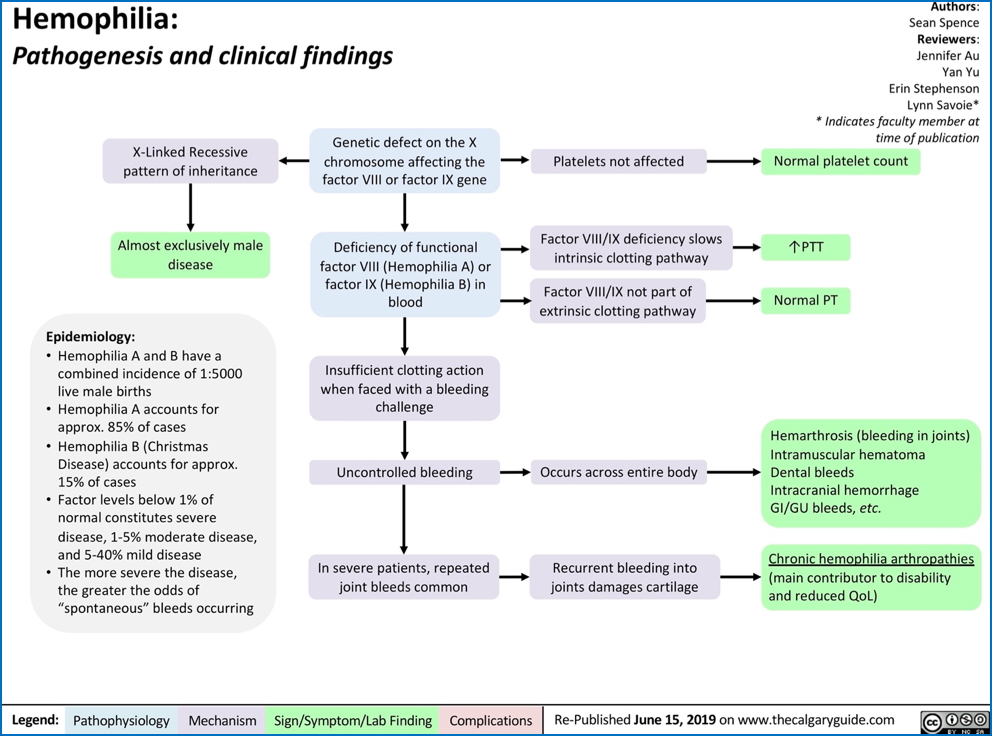
Haemophilia A and B are inherited bleeding disorders caused by deficiencies of clotting Factor VIII and Factor IX, respectively. These conditions lead to impaired coagulation and spontaneous bleeding, particularly into joints and muscles. Haemophilia A is significantly more common than Haemophilia B, and both are inherited in an X-linked recessive pattern, predominantly affecting males. Early diagnosis and regular treatment with recombinant clotting factors are key to preventing complications.
Definition
Haemophilia is a group of hereditary bleeding disorders characterised by a deficiency in specific clotting factors—Factor VIII (Haemophilia A) or Factor IX (Haemophilia B)—resulting in prolonged bleeding times and poor clot formation.
Aetiology
- Inheritance Pattern:
- X-linked recessive
- Typically affects males, while females are carriers and may exhibit mild symptoms due to random X-inactivation
- Haemophilia A (Factor VIII deficiency):
- Accounts for ~80% of haemophilia cases
- More severe phenotype
- Haemophilia B (Factor IX deficiency):
- Also known as Christmas Disease
- Less common (~20% of cases)
Pathogenesis
- Normal Haemostasis:
- Requires a cascade of clotting factors to form stable fibrin clots
- In Haemophilia:
- Deficiency of Factor VIII or IX disrupts the intrinsic coagulation pathway
- → Failure to generate thrombin and fibrin clots
- → Poor haemostasis → spontaneous or trauma-induced bleeding
- Clinical Consequences:
- Severe bruising
- Joint haemorrhages (haemarthroses)
- Muscle bleeds
- Prolonged bleeding after injury or surgery
Clinical Features
- Typically present in infancy or early childhood
- Symptoms:
- Easy bruising
- Spontaneous joint bleeds (haemarthroses)
- Muscle haematomas
- Delayed bleeding after trauma or surgery
- Females (carriers):
- Usually asymptomatic
- May have mild bleeding tendencies
Investigations
- Coagulation studies:
- ↑ Activated partial thromboplastin time (aPTT)
- Normal prothrombin time (PT)
- ↓ Factor VIII or IX activity
- Genetic testing:
- Identifies mutation in F8 or F9 gene
- Carrier testing and prenatal diagnosis available for at-risk families
Management
- Mainstay treatment:
- Regular infusions of recombinant clotting factors (either Factor VIII or IX)
- Prophylactic regimens administered every 1–3 weeks
- Historical treatments (no longer standard):
- Blood transfusions
- Plasma-derived clotting factors (now largely replaced due to risk of viral transmission)
- Heat-treated clotting factors
- Additional Management:
- Desmopressin (mild haemophilia A) to stimulate endogenous Factor VIII
- Avoidance of NSAIDs and IM injections
- Physiotherapy to prevent joint damage
- Haematology specialist follow-up
Prognosis
- Excellent prognosis with early diagnosis and access to recombinant therapies
- Without treatment, repeated joint bleeds can lead to chronic arthropathy
- Life expectancy near normal with comprehensive care
Summary – Haemophilia A & B
Haemophilia A and B are X-linked recessive bleeding disorders resulting from deficiencies in Factor VIII and IX, respectively. Most cases affect males, with symptoms such as spontaneous joint and muscle bleeding. Management involves regular administration of recombinant clotting factors to prevent complications. For a broader context, see our Genetics & Cancer Overview page.