Table of Contents
Overview – Bleeding Disorders
Bleeding disorders are a group of conditions that affect the body’s ability to form blood clots effectively, leading to prolonged or excessive bleeding. These disorders may be due to problems with blood vessels, platelets, coagulation factors, or a combination of all three. Recognising the underlying cause is essential to guide diagnosis and appropriate treatment. This topic serves as a foundation for understanding inherited and acquired haemostatic pathologies.
Classification of Bleeding Disorders
1. Vascular Disorders
- Structural defects in blood vessel walls or surrounding connective tissue
- → Leads to easy bruising, mucocutaneous bleeding
- Often not associated with platelet or coagulation factor abnormalities
2. Platelet Disorders
a) Thrombocytopenia
- Low platelet count
- Causes:
- ↓ Production (e.g., marrow failure, drugs)
- ↑ Destruction (e.g., ITP, DIC, autoimmune)
- ↑ Consumption (e.g., severe trauma, burns)
b) Platelet Dysfunction
- Normal platelet count, but platelets don’t function correctly
- Causes:
- Inherited (rare)
- Acquired (e.g., aspirin, NSAIDs)
3. Von Willebrand Disease (vWD)
- Most common inherited bleeding disorder
- Deficiency or dysfunction of von Willebrand Factor (vWF)
- vWF required for platelet adhesion and to stabilise Factor VIII
- → Results in prolonged bleeding time despite normal platelet count
4. Coagulopathies (Clotting Factor Deficiencies)
a) Hereditary
- Haemophilia A – Factor VIII deficiency
- X-linked recessive (affects males)
- Treated with recombinant Factor VIII
- Haemophilia B – Factor IX deficiency (Christmas disease)
- Also X-linked
- Treated with recombinant Factor IX
- Other rare deficiencies: Factors V, VII, X, XI, XIII
b) Acquired
- Vitamin K Deficiency
- ↓ Factors II, VII, IX, X
- Causes: poor diet, malabsorption, long-term warfarin
- Chronic Liver Disease
- Reduced synthesis of clotting factors & fibrinogen
- Also affects fat-soluble vitamin absorption
- DIC (Disseminated Intravascular Coagulation)
- Pathological widespread clotting → consumption of platelets & factors
- Results in bleeding + thrombosis
Evaluation of Bleeding Disorders
Platelet Count
- Normal range: 150–400 × 10⁹/L
- ↓ Platelet count = thrombocytopenia
Platelet Function Tests
- CBC/FBE: for platelet count and morphology
- Bleeding Time:
- ↑ Bleeding time suggests platelet dysfunction or vWD
- Platelet Aggregometry:
- Measures aggregation response to ADP, epinephrine, collagen
Coagulation Factor Tests
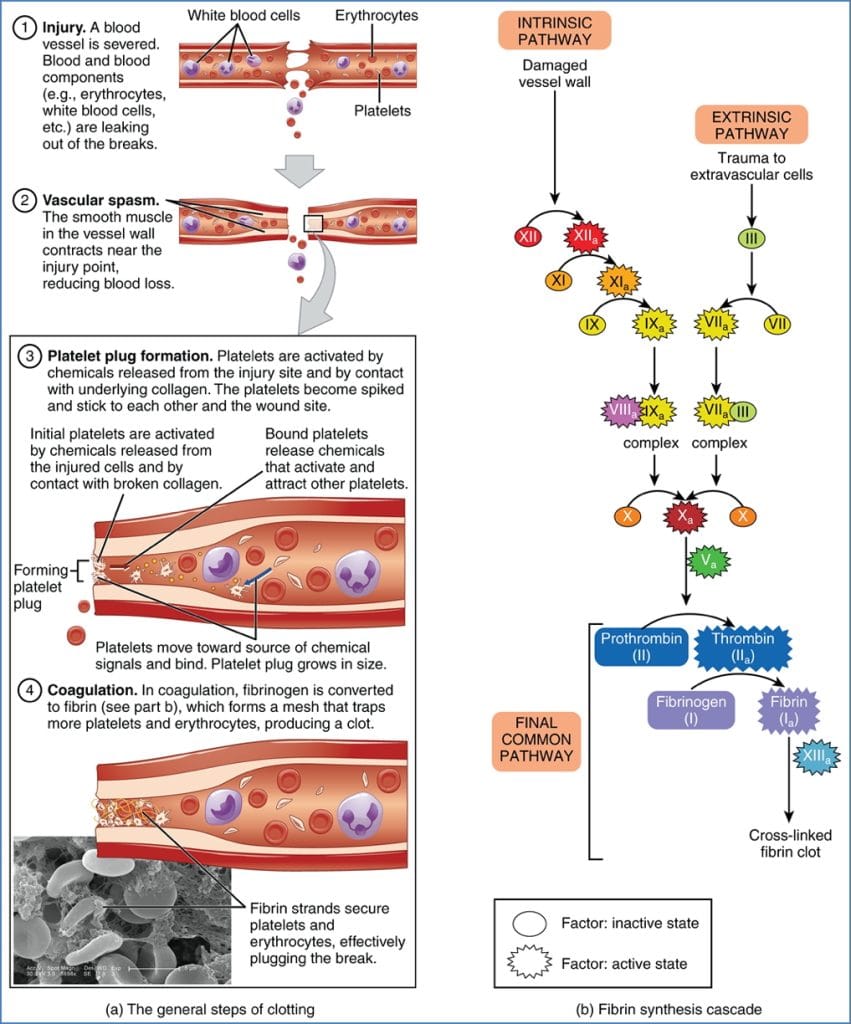
Prothrombin Time (PT)
- Measures extrinsic pathway
- Factors VII, X, V, II, I
- Normal: 12–15 sec
- INR used for standardised comparison
Activated Partial Thromboplastin Time (aPTT)
- Measures intrinsic + common pathway
- Factors XII, XI, IX, VIII, X, V, II, I
- Normal: 25–45 sec
Thrombin Time (TT)
- Evaluates final step: fibrinogen → fibrin
- Assesses fibrinogen deficiency or thrombin inhibition
Summary – Bleeding Disorders
Bleeding disorders can result from vascular defects, thrombocytopenia, platelet dysfunction, vWD, or coagulation factor deficiencies. Evaluation includes platelet counts, coagulation times, and function-specific testing. Early diagnosis and targeted therapy are essential to prevent complications. For a broader haematological context, see our Blood & Haematology Overview page.