Table of Contents
Overview – Gastrointestinal Motility
Gastrointestinal motility refers to the coordinated muscular contractions and relaxations that move food through the digestive tract. This process ensures that food stays in specific segments long enough for optimal digestion and nutrient absorption, and culminates in defecation. Understanding GI motility is crucial for recognising disorders like gastroparesis, constipation, and dysphagia.
General Principles of GI Motility
- Transit Times (Approximate):
- Oesophagus: 5–10 seconds
- Stomach: 1–3 hours
- Small Intestine: 7–9 hours
- Large Intestine: 25–30 hours
- Total GI transit: ~40 hours
- Muscle Actions:
- Contraction:
- Mechanical digestion
- Promotes epithelial contact for absorption
- Propels contents
- Maintains compartmentalisation via sphincters
- Relaxation:
- Accommodates food boluses
- Crucial for peristalsis and swallowing
- Facilitates sphincter opening
- Contraction:
Types of Motility
1. Accommodation
- Stretch-induced relaxation (e.g., in the stomach)
2. Tonic Contraction
- Sustained partial contraction for tone and sphincter control
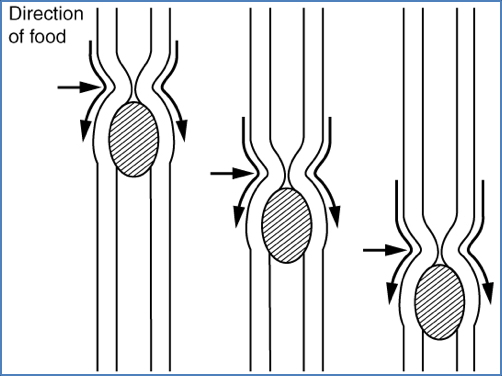
3. Peristalsis
- Coordinated waves of contraction
- Present in oesophagus and stomach
- Involves both segmentation and pendular contractions
- Segmentation:
- Circular muscle contractions
- Mixes contents bidirectionally
- Enhances absorption
- Pendular Contractions:
- Longitudinal muscle contractions
- Shorten and lengthen intestinal segments
- Caterpillar-like motion
- Segmentation:
4. Migrating Motor Complex (MMC)
- Occurs in fasting state
- Originates in duodenum
- Sweeps residual contents toward ileocecal valve
- Regulated by motilin
- Takes ~2 hours per cycle
5. Mass Movements
- Strong, slow, sweeping waves
- Occur 2–3x daily
- Propel colonic contents toward rectum
6. Defecation Reflex
- Triggered by rectal distension
- Involves reflex contraction of sigmoid colon and rectum
- Internal anal sphincter relaxes
- External sphincter under voluntary control
- If delayed, reflex subsides but reinitiates with next mass movement
Region-Specific Motility Mechanisms
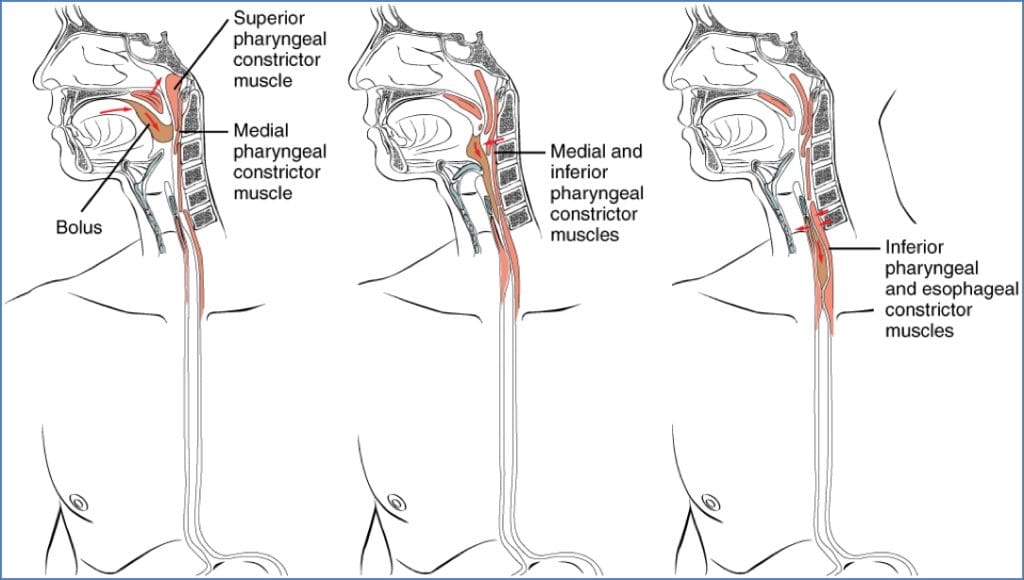
Oesophagus
- Peristalsis initiates swallowing
- Buccal Phase (Voluntary):
- Tongue pushes bolus into oropharynx
- Pharyngeal-Oesophageal Phase (Involuntary):
- Controlled by brainstem (swallowing centre)
- Upper oesophageal sphincter relaxes
- Peristaltic wave propels food downward
- Lower oesophageal sphincter relaxes → food enters stomach
- Buccal Phase (Voluntary):
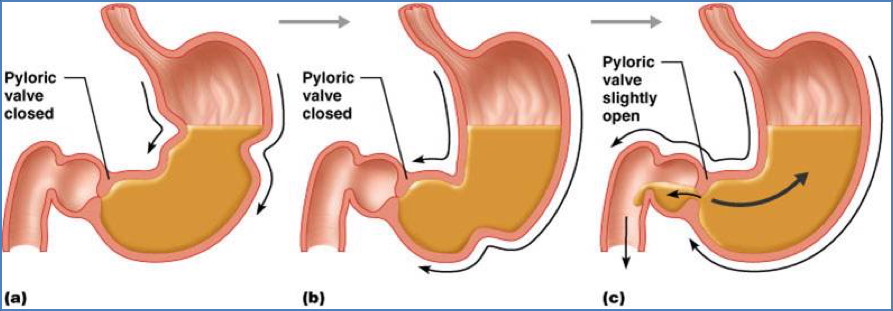
Stomach
- Peristaltic waves begin at the fundus
- Controlled by Cajal cells (pacemakers)
- Occur at ~3/min
- Waves intensify toward the pylorus
- Each wave propels ~3mL of chyme into duodenum
- Remaining chyme is churned further for next wave
Small Intestine
- Primary movement = Segmentation
- ~12–14 contractions/min
- Ensures maximal contact with absorptive mucosa
- MMC (Migrating Motor Complex):
- Begins after nutrient absorption
- Initiated by motilin
- Clears residual matter and bacteria
- Progresses in ~2 hour cycles

Large Intestine
- Low baseline activity
- Stimulated after meals (gastrocolic reflex)
- Mass Movements:
- Long-range peristalsis
- Trigger defecation reflex
- Push contents to rectum
Rectum and Anus
- Faeces enter rectum via mass movements
- Stretch receptors trigger the defecation reflex
- Internal sphincter relaxes (involuntary)
- External sphincter controlled voluntarily
- If delayed, reflex dissipates and restarts later
Summary – Gastrointestinal Motility
Gastrointestinal motility involves complex, region-specific muscle contractions that enable digestion, absorption, and excretion. Key patterns include peristalsis, segmentation, migrating motor complexes, and mass movements. The defecation reflex marks the final step in GI transit. For a broader context, see our Gastrointestinal Overview page.