Table of Contents
Overview – Shoulder Examination
The shoulder examination is a fundamental OSCE skill used to evaluate joint integrity, range of motion, and common shoulder pathologies such as rotator cuff tears, impingement syndrome, adhesive capsulitis, and shoulder instability. By combining inspection, palpation, movement testing, and special maneuvers, clinicians can localize the pathology to specific muscles, joints, or nerves. This guide outlines a high-yield approach to the shoulder examination, including key anatomical landmarks, movement assessments, and special tests relevant for medical students and OSCE candidates.
Definition
The shoulder examination is a structured clinical assessment aimed at identifying musculoskeletal, neurological, or inflammatory causes of shoulder pain and dysfunction. It includes inspection, palpation, active/passive movements, and special tests.
Preparation
- Wash hands, introduce yourself, confirm patient identity.
- Explain the examination and gain consent.
- Ensure the patient is standing with chest and shoulders exposed.
- Look around for walking aids or medication clues (e.g. steroids for PMR).
Inspection
Observe the shoulders anteriorly, laterally, and posteriorly:
- Swelling and erythema → Inflammation (e.g. RA, septic arthritis, bursitis)
- Ecchymosis → Trauma, tendon rupture
- Asymmetry or deformity
- Muscle atrophy:
- Deltoid flattening → Axillary nerve injury (e.g. anterior dislocation)
- Supraspinatus/infraspinatus wasting → Chronic rotator cuff tear
- Posture abnormalities → Elevated shoulder in scoliosis
- Scars → Shoulder replacement, arthroscopy
- Fracture signs → Clavicle deformity
- Popeye sign → Biceps tendon rupture
- Winged scapula (Wall push-up test) → Long thoracic nerve injury (e.g. trauma, lymph node dissection)
Palpation
- Temperature – Assess anterior and posterior shoulder (use back of hand)
- Tenderness – Palpate for patient discomfort
- Bony landmarks to palpate:
- Sternoclavicular joint (SCJ)
- Clavicle
- Acromioclavicular joint (ACJ)
- Acromion
- Coracoid process (2 cm medial/inferior to clavicle tip)
- Spine and borders of scapula
- Head of humerus
- Bicipital groove – Tender in biceps tendinitis
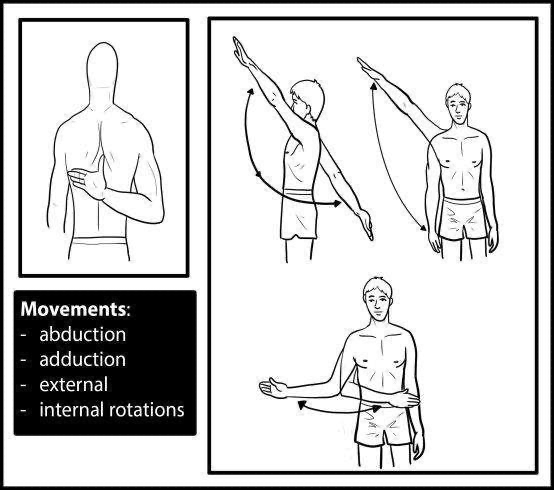
Range of Motion
Assess active, then passive range of motion:
- Flexion: 0–180°
- Extension: 0–60°
- Abduction: 0–180°
- First 15°: Supraspinatus
- 15–90°: Deltoid
- 90–180°: Deltoid + Serratus anterior (scapulohumeral rhythm 1:2)
- Adduction: 0–40°
- External rotation: 0–90°
- Internal rotation: 0–90°
Observe for pain, crepitus (place hand over joint during passive movement), and reduced range.
Special Tests
Impingement Syndrome
- Hawkins Test: Shoulder and elbow at 90°, passively internally rotate → pain = positive
- Neer Test: Internally rotate arm, passively flex → pain = positive
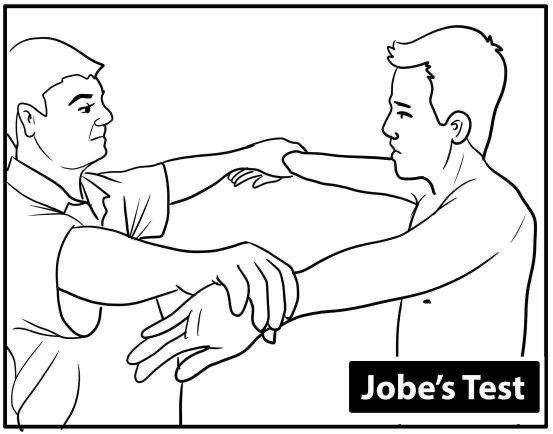
Rotator Cuff Assessment
- Empty Can (Jobe) Test: 90° forward flexion + 30° abduction, thumbs down → resistance against upward force → pain = supraspinatus tear
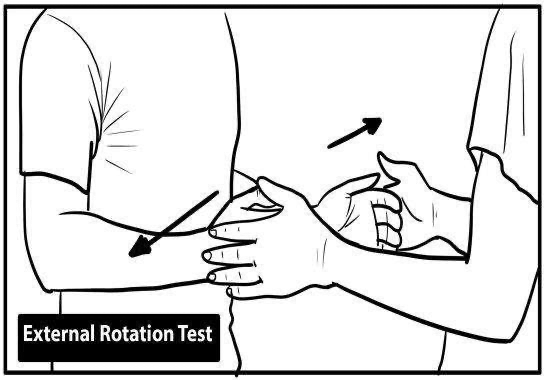
- Infraspinatus/Teres Minor Test: Elbows flexed at 90°, resist external rotation → pain = infraspinatus/teres minor
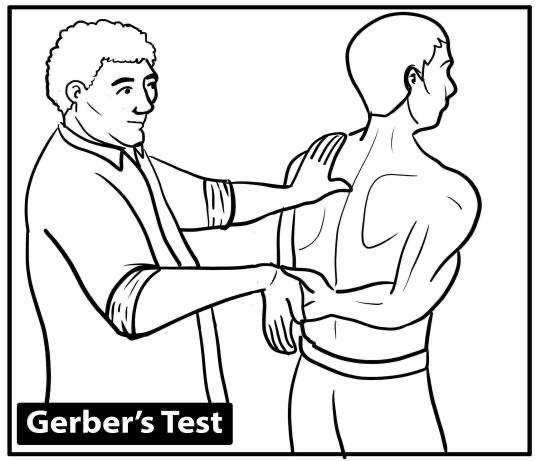
- Gerber Lift-Off Test: Dorsum of hand on back, lift off against resistance → subscapularis involvement
Shoulder Instability
- Apprehension Test (Crank): Patient supine, abduct arm and externally rotate → pain = anterior instability
AC Joint Pathology
- Cross-Body Adduction Test: Elevate arm to 90°, adduct across body → pain = AC joint injury

Rotator Cuff Muscles – “SITS”
- Supraspinatus – Abduction (first 15°)
- Infraspinatus – External rotation
- Teres Minor – External rotation
- Subscapularis – Internal rotation
Common Shoulder Pathologies
1. Impingement Syndrome
- Cause: Compression of rotator cuff tendons (esp. supraspinatus) and subacromial bursa
- Risk Factors: Osteophytes (elderly), repetitive overhead motion (young)
- Features:
- Dull anterolateral pain
- Worse with overhead activity and at night
- Painful arc (60°–120°)
- Positive Hawkins and Neer tests
- Management:
- Physiotherapy
- NSAIDs
- Subacromial steroid injection
- Arthroscopic subacromial decompression (ASD)
2. Frozen Shoulder (Adhesive Capsulitis)
- Risk Factors: Diabetes, hyperthyroidism, immobilization
- Features:
- Global restriction of both active and passive ROM
- Early loss of external rotation
- Three stages: Freezing (painful), Frozen (stiff), Thawing (improving)
- Management:
- NSAIDs
- Physiotherapy
- Intra-articular steroids
- Surgery (capsular release)
3. Polymyalgia Rheumatica (PMR)
- Demographics: Elderly females
- Features:
- Bilateral shoulder and hip girdle pain + stiffness
- Worse at rest, improves with use
- May have systemic symptoms (fever, weight loss)
- Often associated with temporal arteritis
- Elevated ESR
- Management:
- Low-dose corticosteroids (prompt response is diagnostic)
Additional Considerations
- Neurological Exam – To assess for axillary, long thoracic, or suprascapular nerve lesions
- Spurling’s Test – Reproduction of arm pain with neck extension and rotation → suggests cervical radiculopathy
- Adson’s Test – Thoracic outlet syndrome (check for loss of radial pulse with neck rotation and inspiration)
- Investigations:
- X-ray (fracture, joint space narrowing)
- MRI (rotator cuff tear, impingement)
- ESR/CRP (inflammatory markers)
Summary – Shoulder Examination
The shoulder examination is a high-yield OSCE skill for evaluating joint pain, restricted range of motion, and rotator cuff injuries. Combining movement assessments and special tests such as the Hawkins, Neer, and Empty Can tests allows accurate localisation of pathology. For a broader context, see our OSCE Prep Overview page.