Table of Contents
Overview – Airway Hypersensitivity and Asthma
Airway hypersensitivity and asthma is a chronic inflammatory condition marked by airway hyperresponsiveness to a variety of triggers. This topic explores smooth muscle physiology, autonomic and immune influences, pathogenesis of atopic and non-atopic asthma, key diagnostic findings, and stepwise pharmacologic treatment. Includes first aid protocols for acute attacks and comparisons with COPD.
Airway Smooth Muscle & Autonomic Control
Airway Smooth Muscle
- Regulates airway diameter via bronchoconstriction/bronchodilation.
- Prominent in non-cartilaginous airways (bronchioles almost entirely smooth muscle).
- Spasm reduces airway calibre → increased resistance to airflow.
Autonomic Effects
- Sympathetic (β-adrenergic):
- β₂-receptor activation → bronchodilation.
- Example: Salbutamol (Ventolin) = β-agonist.
- Direct sympathetic innervation sparse → most effects from circulating adrenaline.
- Parasympathetic (M3-muscarinic):
- Vagal stimulation → M3 receptor activation → bronchoconstriction.
- Immune/irritant effects:
- Leukotrienes, histamine, and environmental irritants (dust, smoke, perfume) also trigger bronchoconstriction.
Asthma
Definition
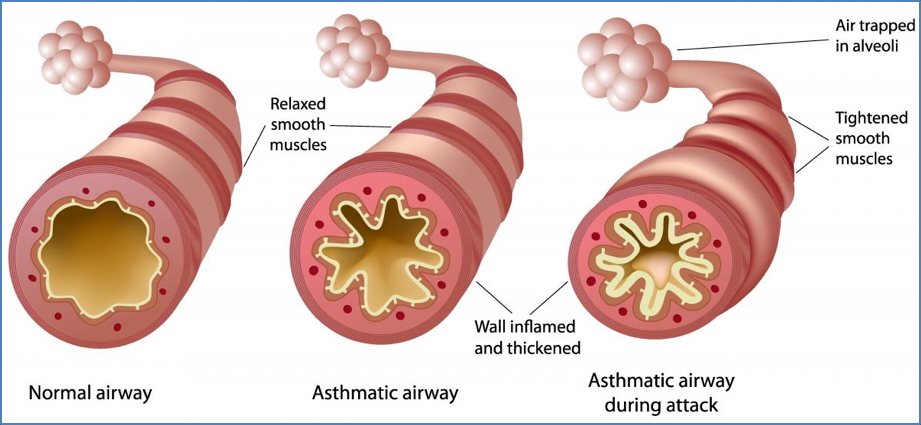
- Hypersensitivity of airways → chronic inflammation → reversible obstruction.
- Pathological changes:
- Narrowed airway lumen.
- Oedematous mucosa.
- Hypertrophied glands → thick mucus.
- Hypertrophied and hyper-reactive smooth muscle.
- Overall: ↑ resistance and obstruction.
Aetiology
- Atopic (allergic) asthma: IgE-mediated (Type I hypersensitivity).
- Non-atopic asthma: Viral, drug-induced, or occupational.
- Triggers: Dust, pollen, animal dander, mould, smoke, pollution, perfume, cold air.
- Genetics: Strong family history association.
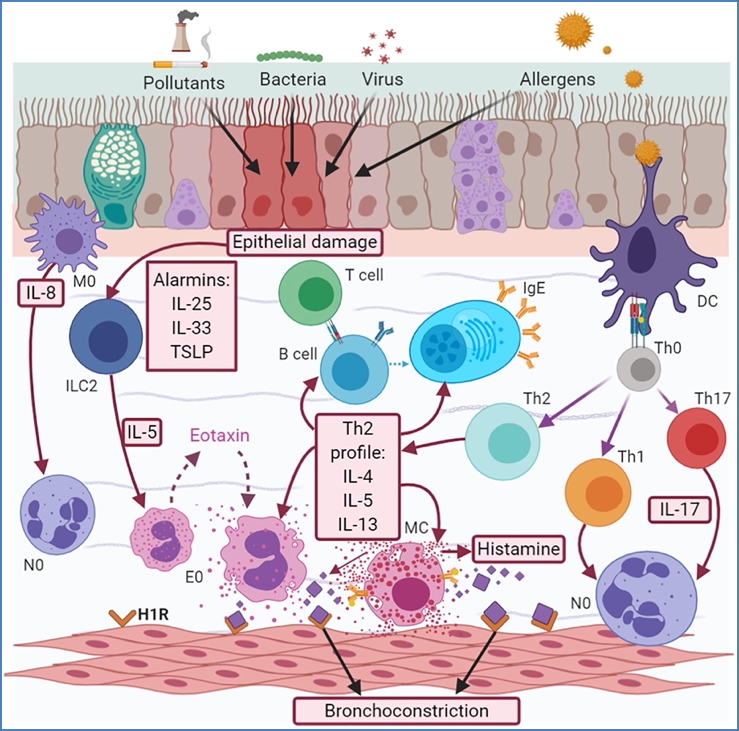
Pathophysiology – Type I Hypersensitivity
Sensitisation Phase:
- Antigen exposure → presented by APC to TH2-helper T cells.
- TH2 release cytokines → activate B cells.
- B cells produce IgE antibodies.
- IgE binds mast cells.
Re-exposure Phase:
- Antigen cross-links IgE on mast cells.
- Mast cell degranulation → release of histamine, leukotrienes, prostaglandins.
Phases of Asthma Attack:
- Early Phase (minutes):
- Mucus hypersecretion.
- Increased vascular permeability → oedema.
- Smooth muscle spasm → bronchoconstriction.
- Late Phase (hours):
- Infiltration of eosinophils, neutrophils, basophils.
- Eosinophils release major basic protein → epithelial damage.
- ↓ mucociliary clearance → mucus plugging.
- ↑ airway responsiveness.
Clinical Features
- Asymptomatic between attacks.
- Asthma attack:
- Severe dyspnoea, wheeze, cough, chest tightness.
- Triggered by allergen exposure or irritants.
- Dynamic airway compression:
- Reliance on forced expiration.
- Equal pressure point moves into unsupported airways → gas trapping.
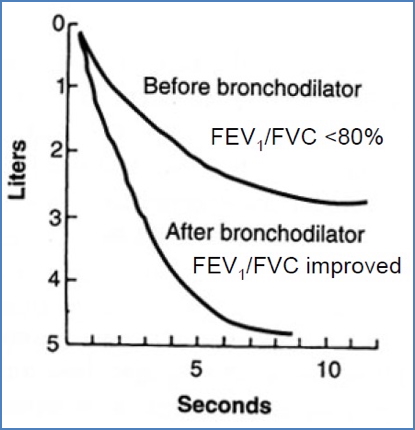
- Investigations:
- ↓ FEV1, ↓ PEFR.
- ↑ RV (air trapping, hyperinflation).
- ↓ arterial PO₂ (V/Q mismatch).
- Bronchodilator response:
- Asthma improves with β₂-agonists.
- COPD generally does not.
- Status asthmaticus: Severe, life-threatening asthma unresponsive to therapy.
Non-Atopic Asthma Variants
- Viral-induced asthma:
- Viral infection lowers vagal threshold → ↑ parasympathetic bronchoconstriction.
- Drug-induced asthma:
- Aspirin → shunts arachidonic acid metabolism → ↑ leukotrienes → bronchospasm.
- Opioids (codeine, morphine), bee venom → mast cell activation.
- Occupational asthma:
- Fumes, gases, dusts.
- Mechanisms: IgE hypersensitivity OR direct irritant effects.
- Exercise-induced asthma:
- Possibly due to airway cooling/drying; mechanism unclear.
Drugs Used in Asthma
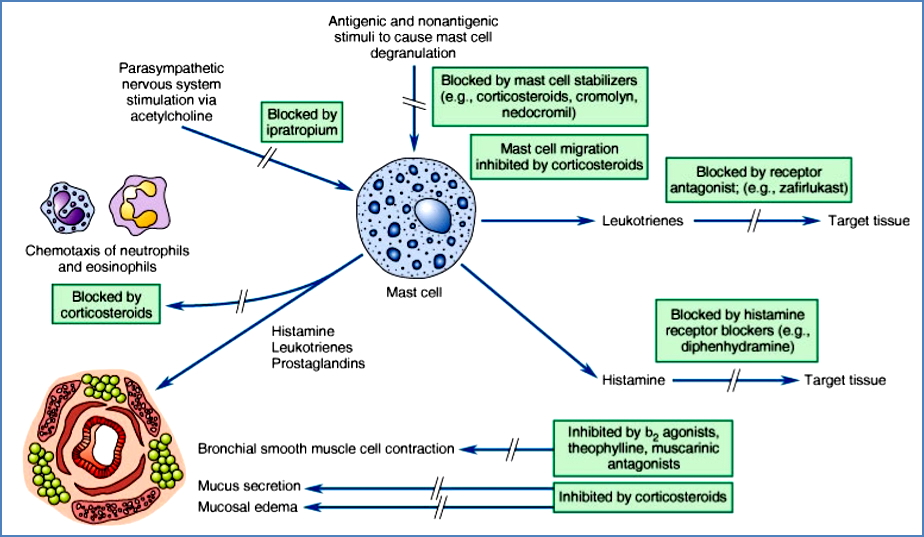
1. Bronchodilators
- β₂-agonists:
- Stimulate β₂ receptors on smooth muscle → bronchodilation.
- Stabilise mast cells → inhibit mediator release.
- Anticholinergics (e.g. ipratropium):
- Block M3 muscarinic receptors → inhibit vagal bronchoconstriction.
- Less effective than β₂-agonists, but useful in combination.
2. Anti-Inflammatory Drugs
- Corticosteroids:
- Prevent mast cell degranulation.
- Reduce chemotaxis of eosinophils, neutrophils.
- ↓ mucus secretion, ↓ mucosal oedema.
- ↑ β-receptor expression.
- Inhibit cytokine release.
Delivery
- Inhalers: convenient, lower doses.
- Nebulisers: higher doses; used in acute attacks.
Clinical Management
Prevention
- Mild asthma: inhaled corticosteroids (ICS) – e.g. budesonide, fluticasone.
- ICS-intolerant: inhaled antimuscarinic (ipratropium).
- Moderate asthma: LABA + ICS combinations (e.g. Symbicort, Seretide).
- Severe asthma: leukotriene inhibitors (montelukast).
Acute Attack (Adults & Children)
- Oxygen if SpO₂ <92%.
- Salbutamol (Ventolin): via spacer (pediatric: <6 puffs if <6yo, <12 puffs if >6yo; adult: up to 12 puffs).
- If severe → add ipratropium bromide.
- Add systemic corticosteroids (PO prednisolone).
- If refractory → IV magnesium sulfate or IV aminophylline.
- Escalate to ICU if unresponsive.
Example Asthma Action Plan
- Severe symptoms: frequent salbutamol (every 15–30 min). Call ambulance if not improving.
- Prophylaxis: montelukast at night.
- Mild symptoms: salbutamol 2 puffs as needed.
- Moderate symptoms: salbutamol 6 puffs + prednisolone.
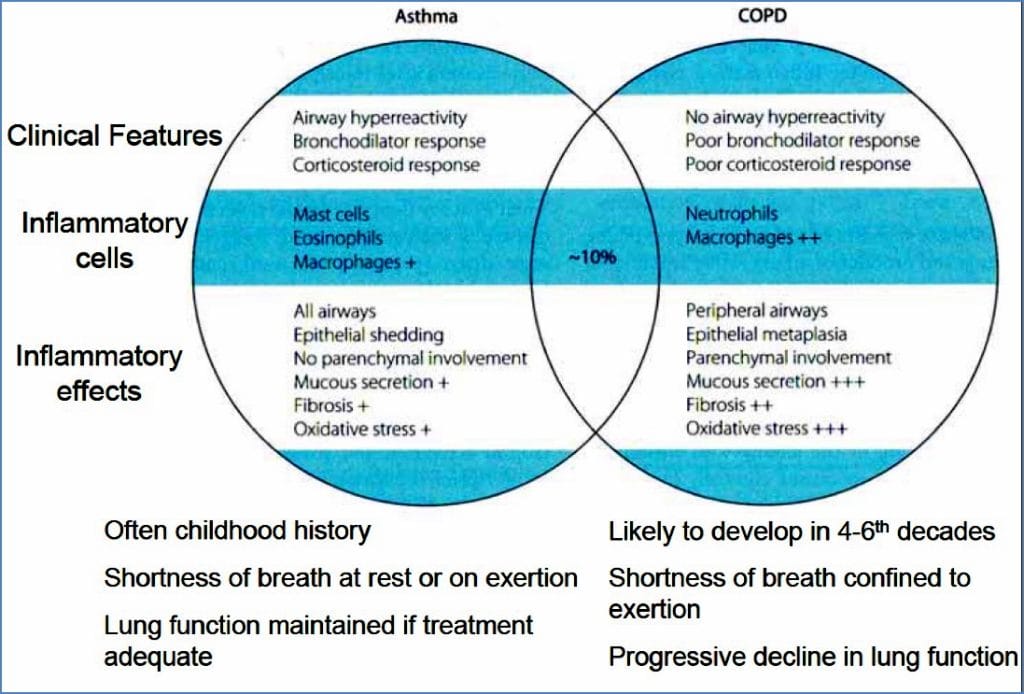
Asthma vs COPD
- Asthma: episodic, reversible, inflammatory, responsive to bronchodilators.
- COPD: progressive, irreversible, usually non-responsive to bronchodilators.
Summary – Airway Hypersensitivity and Asthma
Airway hypersensitivity and asthma are characterised by reversible bronchoconstriction caused by inflammation, smooth muscle hyperreactivity, and mucosal oedema. Clinical diagnosis relies on symptoms and spirometry, with reversibility distinguishing asthma from COPD. Treatment involves bronchodilators, anti-inflammatory agents, and personalised prevention strategies. Severe acute attacks require escalation to systemic therapy and, in refractory cases, intensive care. For a broader context, see our Respiratory Overview page.