Table of Contents
Overview – Retained Placenta
Retained placenta refers to the failure of placental delivery within 30 minutes after birth and is a significant cause of postpartum haemorrhage (PPH) and infection. Prompt recognition and management are crucial to prevent serious maternal morbidity. Understanding the pathophysiology, risk factors, and stepwise management of retained placenta is essential for final-year medical students preparing for clinical rotations and exams.
Definition
- Retained placenta is defined as failure to deliver the placenta within 30 minutes following the birth of the baby.
- It is considered an obstetric emergency due to the risk of severe bleeding and infection.
Aetiology
Retained placenta is typically due to abnormal placental adherence or separation:
- Placenta accreta – attachment to the myometrium without invasion
- Placenta increta – partial invasion into the myometrium
- Placenta percreta – full penetration through the uterine wall
Risk Factors
- Placenta praevia
- Previous caesarean section
- Uterine infection (e.g. chorioamnionitis)
Clinical Features
- Delayed placental delivery (>30 minutes)
- Increased risk of postpartum haemorrhage
- Fever or signs of uterine infection
- Incomplete uterine contraction
Investigations
- Manual exploration of the uterus (usually in theatre or with adequate analgesia)
- Ultrasound may assist in identifying retained placental tissue, especially in cases of suspected morbid adherence
Management
Initial Resuscitation
- Insert two large-bore IV cannulae
- Perform blood group and crossmatch in anticipation of transfusion
Non-surgical Measures
- Brant manoeuvre:
- Controlled cord traction with suprapubic pressure to prevent uterine inversion
- Umbilical vein injection of oxytocin to stimulate uterine contraction
Surgical Intervention
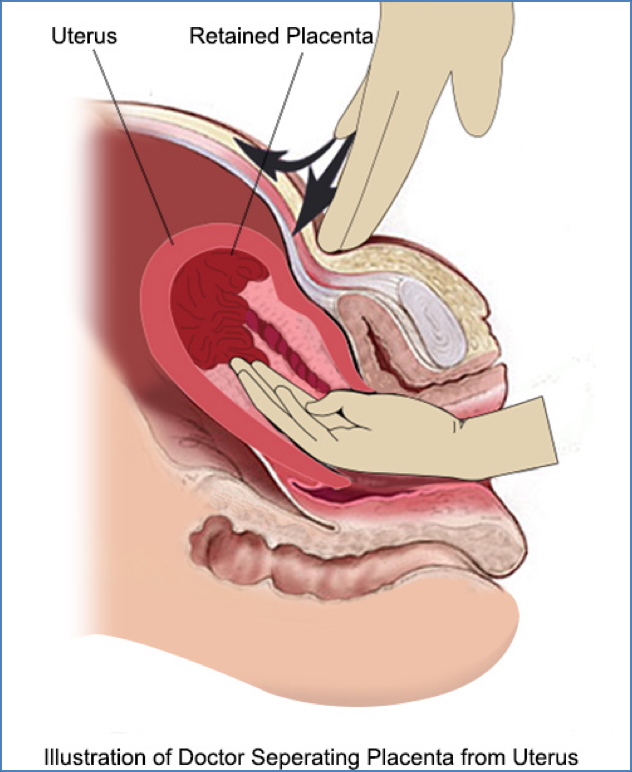
- Manual removal of placenta under appropriate analgesia or anaesthesia
- Dilation and curettage (D&C) if removal is incomplete or bleeding persists
Summary – Retained Placenta
Retained placenta, defined as failure to deliver the placenta within 30 minutes postpartum, can lead to serious complications like postpartum haemorrhage and infection. Risk factors include placenta praevia, prior caesarean section, and uterine infection. Prompt diagnosis and management—including uterotonic administration, manual removal, and surgical intervention when necessary—are key. For a broader context, see our Obstetrics Overview page.