Table of Contents
Overview – Prenatal Screening Tests
Prenatal screening tests are essential components of antenatal care, enabling early identification of fetal anomalies, genetic conditions, and pregnancy complications. These assessments include ultrasound scans, diagnostic procedures like amniocentesis and chorionic villus sampling, and fetal surveillance tools such as the non-stress test. Understanding their timing, indications, and limitations is critical in guiding informed clinical decisions throughout pregnancy.
Ultrasound Screening
8–12 Weeks – Dating Scan
- Accurately estimates gestational age and calculates the estimated due date (EDD)
- Most precise method for pregnancy dating
11–14 Weeks – Nuchal Translucency Scan
- Early screening test for Down syndrome (Trisomy 21)
- Can also detect:
- Cardiac anomalies
- Turner’s syndrome
- Often combined with maternal serum biochemistry (first-trimester combined screening)
18–20 Weeks – Anatomy & Growth Scan
- Mid-trimester morphology scan
- Comprehensive assessment of fetal anatomy
- Detects structural anomalies and assesses fetal growth parameters
Amniocentesis (15–16 Weeks Gestation)
What Is It?
- Ultrasound-guided transabdominal aspiration of amniotic fluid
Why Is It Done?
- Detects chromosomal abnormalities (e.g. Trisomy 21)
- Screens for open neural tube defects
- Confirms abnormalities suggested on ultrasound or non-invasive screening
- Can assess fetal lung maturity via L:S ratio (lecithin:sphingomyelin)
- L:S >2:1 → lower risk of neonatal respiratory distress syndrome
Risks
- ~1 in 200 risk of procedure-related pregnancy loss
- Risk increases (~1 in 100) for multiple gestations

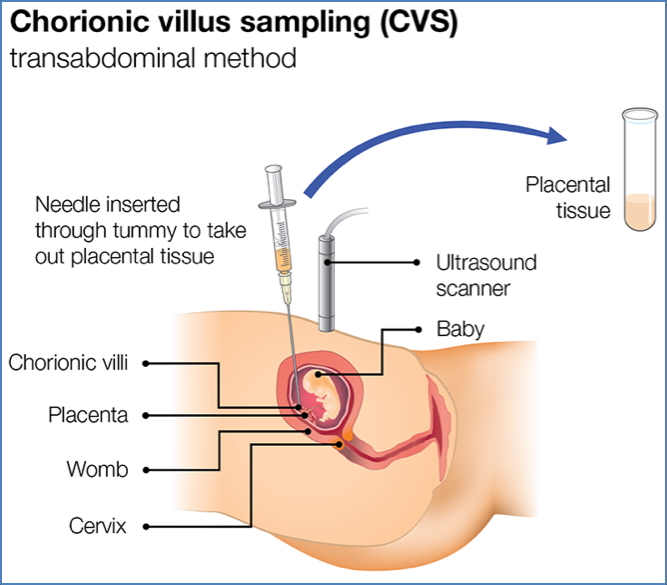
Chorionic Villus Sampling (CVS) (10–12 Weeks Gestation)
What Is It?
- Transcervical biopsy of fetal chorionic tissue
Why Is It Done?
- Detects genetic and chromosomal abnormalities (like amniocentesis)
- Enables earlier diagnosis and potential termination if needed
Risks
- 1–2% risk of procedure-related miscarriage
- 1–2% risk of genetic mosaicism → potential for false negatives

Antenatal Fetal Surveillance
Fetal Movements
- Usually first perceived by the mother at 16–20 weeks
- All high-risk pregnancies require formal fetal movement counting
- Normal: >6 movements in a 2-hour period
- If <6, prompt review by midwife or doctor is recommended
Fetal Non-Stress Test (NST)
Indications
- Evaluates fetal oxygenation and wellbeing
- Typically used in:
- High-risk pregnancies
- Decreased fetal movements
Basic Principle
- A well-oxygenated fetus shows spontaneous heart rate accelerations in response to movement
- Foetal hypoxia blunts this response
Interpretation
Quick Criteria:
- Normal: ≥2 accelerations >15 bpm for >15s within a 20-minute period
- Abnormal: <2 accelerations within 40 minutes
- No accelerations? → Try fetal stimulation (e.g. fundal pressure, vibroacoustic)
Full Criteria (May vary by institution):
Normal / Reactive:
- Baseline FHR: 110–160 bpm
- Moderate variability (5–25 bpm)
- ≥2 accelerations in 20 minutes
- 15 bpm above baseline for >15s if >32 weeks
- 10 bpm for >10s if <32 weeks
- No decelerations
- → Reassuring
Atypical / Non-Reactive:
- FHR 100–110 bpm or >160 bpm for <30 mins
- Absent/minimal variability (40–80 mins)
- Variable decelerations (30–60s)
- → Requires further monitoring or assessment
Abnormal / Non-Reactive:
- FHR <100 or >160 bpm for >30 mins
- Sinusoidal variability (>25 bpm) for >10 mins
- Decelerations >60s
- → Urgent action required: ultrasound or biophysical profile
- May require delivery if no improvement

Summary – Prenatal Screening Tests
Prenatal screening tests play a central role in the early detection of fetal anomalies, guiding decisions about further investigation or intervention. From early ultrasounds to fetal surveillance tools like the non-stress test, these tests form the backbone of evidence-based antenatal care. For a broader context, see our Obstetrics Overview page.