Table of Contents
Overview – Premature Rupture of Membranes
Premature rupture of membranes (PROM) refers to the rupture of the amniotic sac prior to the onset of labour. It is considered a normal variation when occurring at term but can pose significant risks when it happens before 37 weeks, known as preterm PROM (PPROM). The condition is associated with a risk of infection, preterm labour, and neonatal complications, making accurate diagnosis and timely intervention essential.
Definition
- PROM: Rupture of amniotic membranes before the onset of labour at >37 weeks gestation.
- Prolonged PROM: Rupture lasting >18–24 hours before the onset of labour.
- PPROM: PROM occurring before 37 weeks gestation.
Labour usually begins within 48 hours of PROM, but in some cases, the membranes may reseal spontaneously.
Aetiology
Most cases are spontaneous, but PROM and PPROM may be linked to:
Risk Factors
- Infective causes:
- Chorioamnionitis
- Maternal sepsis
- Vaginitis, cervicitis
- Sexually transmitted infections
- Urinary tract infections
- Structural/Anatomical:
- Anomalies of the amniotic sac, uterus, cervix, or fetus
- Cervical incompetence
- Obstetric:
- Multiparity
- Previous PROM or PPROM
- Multiple gestation
- Lifestyle:
- Cigarette smoking
Clinical Features
- Sudden gush of fluid from the vagina
- May be followed by continuous leakage
- Occurs in a pregnant woman, with no active labour contractions
Investigations
- Detailed history and sterile speculum examination
- Look for fluid pooling in the posterior fornix or leakage from the cervical os
- Nitrazine paper test
- Turns blue in contact with alkaline amniotic fluid
- Ultrasound
- Evaluate fetal anatomy and presentation
- Amniotic fluid smear test (fern test)
- Dried fluid shows a characteristic “fern-like” crystallisation pattern under microscopy
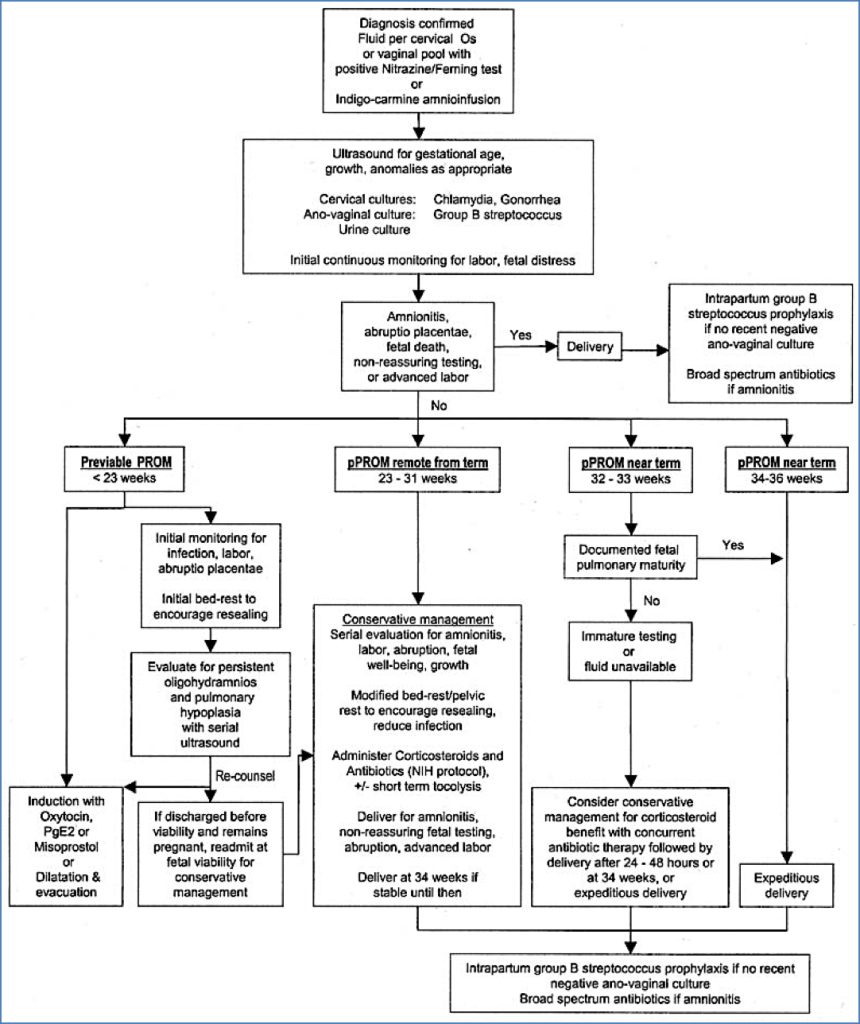
Management
PROM at Term (≥37 weeks)
- Allow up to 12 hours for spontaneous labour to commence
- Induce labour if contractions have not begun by 12 hours
- Consider Group B Streptococcal (GBS) prophylaxis if >18 hours post-rupture or unknown maternal GBS status
PPROM (<37 weeks)
- Admit to hospital for monitoring
- Corticosteroids (e.g. betamethasone) over 2 days to accelerate fetal lung maturity
- Antibiotic prophylaxis (ampicillin + erythromycin) to reduce infection risk and prolong latency
- Monitor closely for signs of:
- Preterm labour
- Chorioamnionitis
- Tocolysis may be considered if <34 weeks gestation and no infection
- Induce labour at 34 weeks if no contraindications
Suspected or Confirmed Infection
- Chorioamnionitis:
- Administer IV antibiotics
- Immediate delivery is usually indicated
- Unknown GBS status:
- Give intrapartum antibiotic prophylaxis to prevent neonatal GBS transmission
Complications
- Maternal:
- Chorioamnionitis
- Endometritis
- Sepsis
- Fetal/Neonatal:
- Preterm birth
- Neonatal sepsis
- Respiratory distress syndrome
- Umbilical cord prolapse
Prognosis
- PROM at 28–34 weeks: ~90% go into labour within one week
- PROM <26 weeks: ~50% go into labour within one week
- Prognosis is significantly improved with corticosteroids and timely delivery
Differential Diagnosis
- Urinary incontinence
- Physiological increased vaginal discharge
- Vaginal infection (causing discharge)
- Cervical incompetence
Summary – Premature Rupture of Membranes
Premature rupture of membranes (PROM) refers to rupture of the amniotic sac before labour begins, and becomes pathological when occurring before 37 weeks (PPROM). Accurate diagnosis, maternal and fetal monitoring, and timely delivery are critical in reducing morbidity. For a broader context, see our Obstetrics Overview page.