Table of Contents
Overview – Obstetric Tumours
Obstetric tumours refer to a group of abnormal growths that arise from placental trophoblastic tissue during or following pregnancy. These include benign conditions like hydatidiform mole and malignant forms such as choriocarcinoma. Prompt diagnosis is critical, as some of these tumours can be highly invasive or metastatic, but are also highly treatable with appropriate therapy.
Hydatidiform Mole
Definition
A hydatidiform mole is a form of gestational trophoblastic disease caused by abnormal fertilisation, resulting in cystic swelling of chorionic villi and trophoblastic hyperplasia. It can be partial or complete, with differing genetic and clinical characteristics.
Aetiology
- Caused by errors in gamete fusion leading to abnormal karyotypes incompatible with life
- Partial Mole:
- Fertilisation of one ovum by two sperms → Triploidy (69 chromosomes)
- Complete Mole:
- Fertilisation of an empty ovum by one sperm (which duplicates) or two sperms → Diploidy (46 paternal chromosomes)
Morphology
Partial Mole
- Macroscopic:
- Partially cystic placental tissue
- Some visible blood vessels
- Microscopic:
- Focal trophoblastic hyperplasia
- Only SOME chorionic villi are cystic
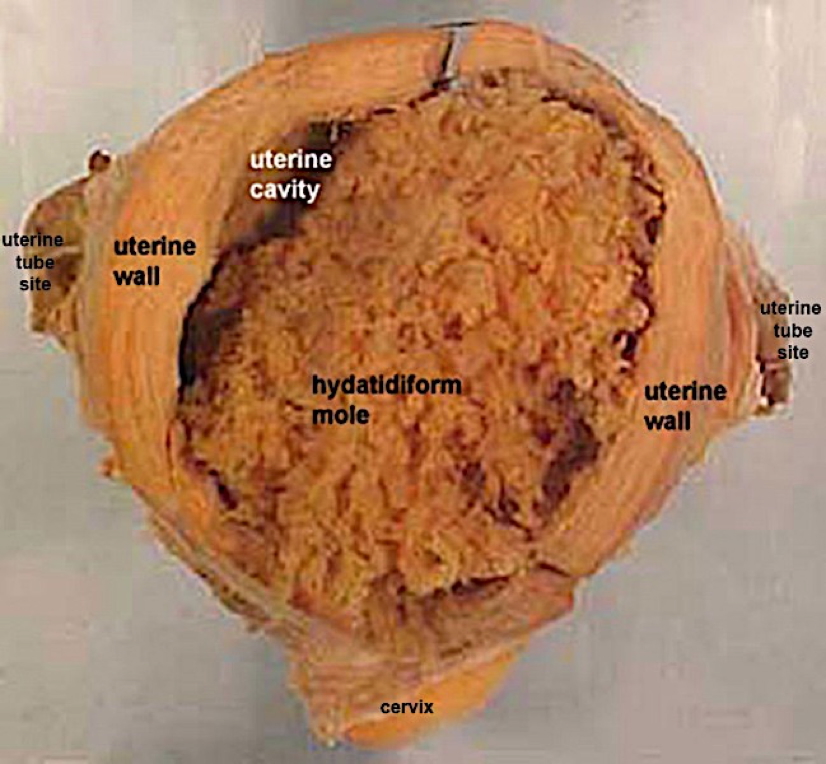
Complete Mole
- Macroscopic:
- All chorionic villi are cystic
- No blood vessels within villi
- Grape-like clusters filling uterine cavity
- Microscopic:
- Diffuse trophoblastic hyperplasia
- ALL chorionic villi are cystic
Clinical Features
- Abnormal uterine enlargement
- Painless vaginal bleeding in the first trimester
- Excessive nausea and vomiting (due to elevated β-hCG)
- Signs of hyperthyroidism (e.g. heat intolerance, tachycardia)
- Early-onset pre-eclampsia (before 20 weeks)
Investigations
- β-hCG:
- Elevated in partial moles
- Markedly elevated in complete moles
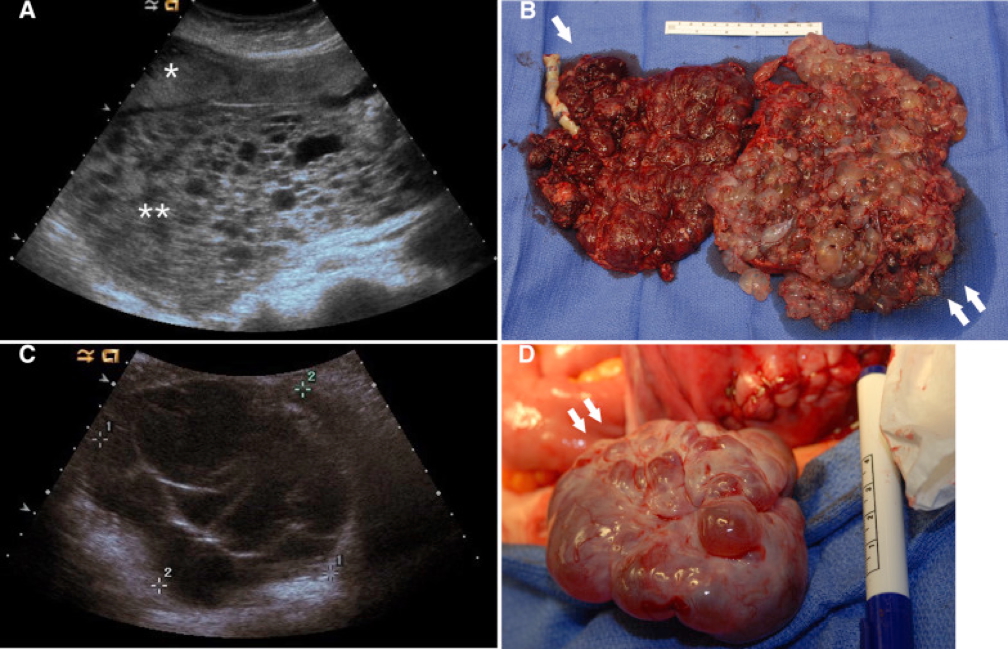
- Pelvic Ultrasound:
- “Snowstorm” or “grape cluster” appearance
- Absence of a viable foetus in complete mole
Management
- Surgical uterine evacuation via suction curettage
- Serial β-hCG monitoring until undetectable
- Contraception advised during follow-up to avoid confusing hCG interpretation
- In cases of persistent trophoblastic disease → Chemotherapy (e.g. Methotrexate)
Complications
- Anaemia, haemorrhage
- Theca lutein cysts
- Persistent gestational trophoblastic neoplasia (GTN)
- Progression to invasive mole or choriocarcinoma in up to 20% of complete moles
Choriocarcinoma
Definition
Choriocarcinoma is a highly malignant form of gestational trophoblastic neoplasia that arises from trophoblastic tissue. It may occur de novo, or more commonly, as a progression from a complete mole.
Aetiology
- Risk factors:
- Maternal age <20 or >40
- History of molar pregnancy
- Previous abortion or abnormal gestation
- May follow complete mole, miscarriage, term pregnancy, or ectopic pregnancy
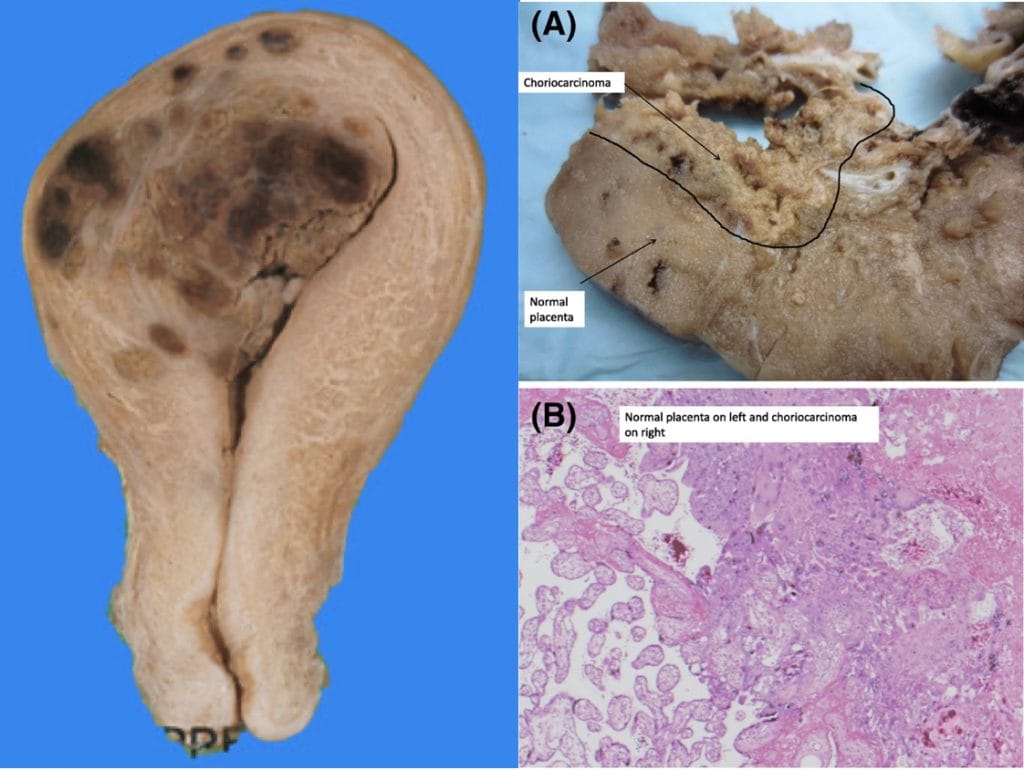
Morphology
- Macroscopic:
- Highly invasive mass
- Often haemorrhagic and necrotic
- Lacks chorionic villi on histology
Clinical Features
- Irregular vaginal bleeding
- Uneven enlargement of uterus
- Abdominal or pelvic pain
- Symptoms related to metastases:
- Commonly lungs → haemoptysis
- Also liver, brain, or vagina
Investigations
- β-hCG: Elevated and rising
- Imaging:
- Pelvic ultrasound
- CT chest/abdomen/pelvis to assess for metastases
Management
- Chemotherapy (Methotrexate ± Actinomycin D)
- Surgical intervention if needed (e.g. hysterectomy in select cases)
- Multidisciplinary team involvement for metastatic disease
Prognosis
- Gestational choriocarcinoma: Excellent prognosis with treatment (near 100% cure rate)
- Non-gestational (gonadal) choriocarcinoma: Poor prognosis
Summary – Obstetric Tumours
Obstetric tumours include hydatidiform moles and choriocarcinoma, both of which originate from abnormal trophoblastic tissue. Hydatidiform moles may be partial or complete and require surgical evacuation and hCG follow-up due to their potential for malignant transformation. Choriocarcinoma is an aggressive but highly treatable malignancy, particularly when caught early. For a broader context, see our Obstetrics Overview page.