Table of Contents
Overview
Gait refers to the process of walking—a complex, coordinated movement requiring precise neuromuscular control. It involves a sequence of joint positions, muscle activations, and biomechanical shifts across different phases. A solid understanding of gait mechanics is crucial for identifying abnormalities due to musculoskeletal, neurological, or structural impairments.
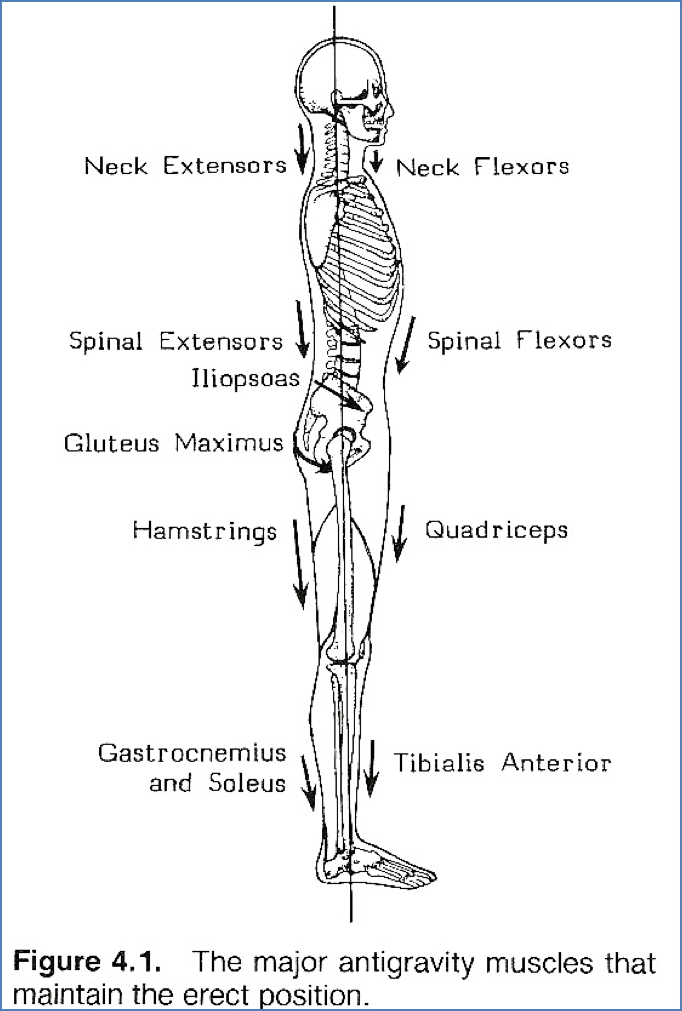
Standing Posture
- Highly energy-efficient: Only 7% more energy than lying down
- Postural muscles maintain alignment
- All three lower limb joints are in their most stable positions:
Hip
- Neutral or extended
- Iliofemoral ligament taut
- Centre of gravity lies posterior to the joint
Knee
- Fully extended
- Ligaments taut
- Centre of gravity lies anterior to the joint
Ankle
- Neutral or slightly dorsiflexed
- No intrinsic stabilisers; stabilised by triceps surae (gastrocnemius + soleus)
- Centre of gravity lies anterior to the joint
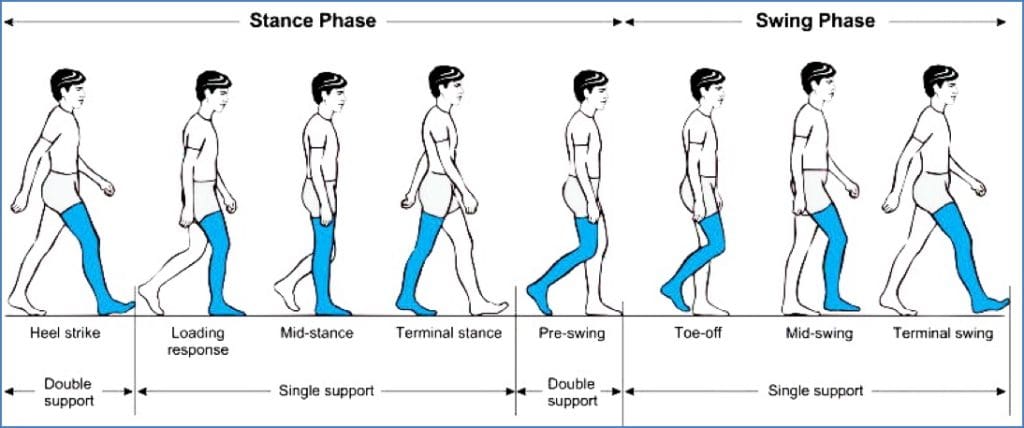
Phases of Gait
1. Stance Phase (Foot is on the ground)
| Phase | Hip Position | Knee Position | Ankle Position | Prime Movers | Stabilisers |
|---|---|---|---|---|---|
| Heel Strike | Flexed | Slightly flexed | Dorsiflexed | Psoas, gravity | Gluteus Maximus, Quadriceps |
| Midstance | Flexed → Neutral | Extended | Neutral/Dorsiflexed | Gluteus Maximus, Hamstrings | Gluteus Medius/Minimus, TFL |
| Toe-Off | Neutral → Flexed | Beginning flexion | Plantarflexed | Triceps surae | Quadriceps, Toe flexors |
2. Swing Phase (Foot is off the ground)
| Motion | Hip Motion | Knee Motion | Ankle Motion | Prime Movers | Stabilisers |
|---|---|---|---|---|---|
| Swing | Extension → Flexion | Flexion → Extension | Dorsiflexion | Iliopsoas, lateral rotators, Tibialis Anterior | Gluteus Maximus (antagonist), Quadriceps, Hamstrings (antagonist) |
Features of Gait
- Centre of Gravity: Lower CoG = greater stability
- Base of Support: Wider base = more stable (e.g. use of walking aids)
- Step Length, Velocity, Cadence: Key measurable parameters
Factors Influencing Gait
- Age/Maturation (adult pattern ~10 years)
- Elderly changes
- Gender differences
- Pain
- CNS disorders: Stroke, Parkinson’s, MS
- Musculoskeletal impairments: Arthritis, injury, joint fusion
- Assistive devices: Braces, orthotics
- Habitual and emotional state
- Terrain and footwear
- Height and body weight
Gait Analysis Methods
- Visual observation (in clinic)
- Video analysis (slow-motion, motion tracking)
- Sensor-based timing tools (e.g. force plates, gait mats)

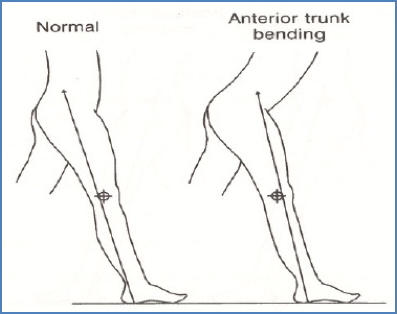
Examples of Gait Abnormalities
Anterior Trunk Bending
- Compensatory forward lean
- Causes: Weak knee extensors, fused knee, tight hip flexors
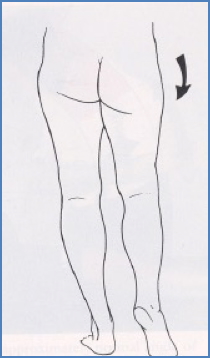
Trendelenburg (Hip Drop)
- Due to gluteus medius/minimus weakness
- Contralateral hip drops during stance
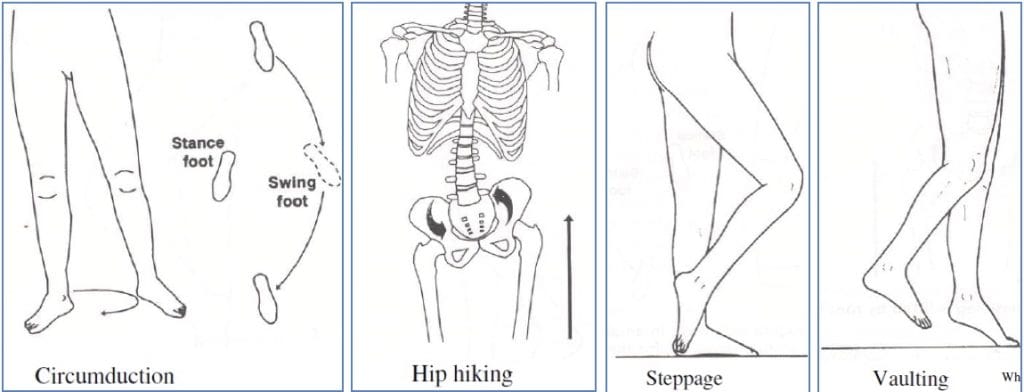
Leg Length Discrepancy
- Anatomical: Bone length difference
- Functional: Due to muscle imbalance or joint dysfunction
- Compensations:
- Hip circumduction
- Hip hiking
- Steppage gait
- Vaulting on contralateral limb
Other Common Issues
- Excessive Knee Extension: Snapping into full extension; often due to weak knee flexors
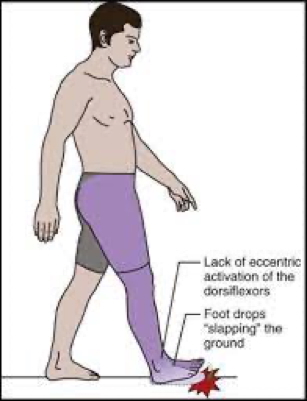
- Foot Slap: Poor eccentric control of dorsiflexors post heel strike
- Toe Drag: Plantarflexed ankle during swing phase due to dorsiflexion failure
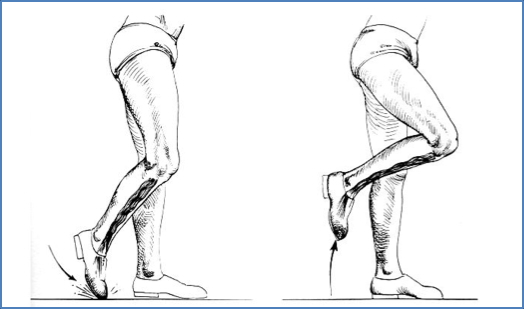
- Insufficient Toe-Off: Entire foot lifts instead of pushing off from toes
- Causes: Achilles tendon injuries, nerve lesions, ankle fusion, forefoot pain
Summary
Gait is a highly coordinated process requiring balanced joint positioning, muscle activation, and postural control. Both stance and swing phases involve specific muscular patterns, with variations in step, cadence, and balance influenced by age, pathology, or terrain. Understanding gait helps clinicians diagnose abnormalities and assess rehabilitation outcomes. For a broader context, see our Musculoskeletal Overview page.