Table of Contents
Overview – Laryngeal Tumours
Laryngeal tumours include a spectrum of benign and malignant lesions affecting the larynx. Benign growths such as vocal cord nodules and recurrent respiratory papillomatosis often present with hoarseness or voice changes. Malignant tumours, most commonly squamous cell carcinoma, are closely linked to smoking and alcohol and require prompt recognition and management. This page outlines the key features of both benign and malignant laryngeal tumours.
Definition
Lesions arising from the laryngeal tissues, ranging from benign inflammatory or viral growths to invasive malignancies.
Aetiology
Benign Tumours
- Vocal Cord Nodules: Chronic irritation (e.g. vocal strain in singers, smoking)
- Recurrent Papillomatosis: HPV infection (vertical transmission from mother to child)
Malignant Tumours
- Squamous Cell Carcinoma (SCC): Strong association with:
- Tobacco use
- Alcohol
- Radiation exposure
- Male gender (M:F ratio ~7:1)
Morphology / Pathophysiology
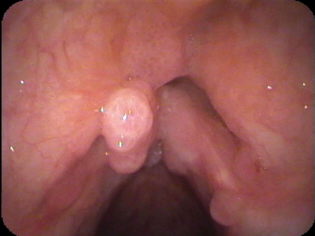
Vocal Cord Nodules
- Fibrous nodules on the true vocal cords
- May be bilateral and symmetrical

Recurrent Papillomatosis
- Warty epithelial growths, typically on the vocal cords
- May extend into the trachea
Laryngeal Carcinoma
- Invasive squamous cell carcinoma
- Commonly arises on the vocal cords (glottic region)
- Can infiltrate surrounding structures if advanced

Clinical Features
Vocal Cord Nodules
- Hoarseness or breathy voice
- History of vocal overuse
- May bleed but non-malignant
Recurrent Papillomatosis
- Presents in childhood
- Hoarseness, stridor, or airway obstruction
- May require repeated surgical intervention
Laryngeal Carcinoma
- Persistent hoarseness (>3 weeks)
- Dysphagia
- Odynophagia
- Sore throat
- Referred otalgia
- Neck mass (late)
- Airway obstruction (advanced)
Investigations
- Laryngoscopy: Direct visualisation of vocal lesions
- Imaging: Head and neck CT or MRI for staging malignant lesions
- Biopsy: Excisional or needle biopsy for histological confirmation
- HPV Testing: For recurrent papillomatosis
Management
Benign Lesions
- Vocal Cord Nodules:
- Voice rest
- Speech therapy
- Surgical excision if persistent
- Recurrent Papillomatosis:
- Surgical debulking (e.g. laser excision)
- Adjuvant antiviral therapies under investigation
Malignant Lesions (Laryngeal SCC)
- Excisional biopsy (grading and diagnosis)
- Laryngectomy (partial or total depending on extent)
- Radiotherapy and/or chemotherapy
- Tracheostomy if airway obstruction is severe
Complications
- Airway obstruction
- Recurrent disease (especially papillomatosis)
- Metastasis (common in advanced SCC)
- Speech impairment (following surgery or tumour progression)
Differential Diagnosis
- Acute laryngitis
- Vocal cord polyps
- Epiglottitis
- Gastroesophageal reflux disease (GERD)
- Tuberculosis or sarcoidosis (if granulomatous appearance)
Summary – Laryngeal Tumours
Laryngeal tumours range from benign vocal cord nodules and HPV-related papillomas to aggressive squamous cell carcinomas. Early signs like hoarseness should not be ignored, particularly in high-risk individuals. Excisional biopsy and imaging guide management, which varies by lesion type. For broader context, visit our Head and Neck Overview page.