Table of Contents
Overview – Cushing’s Syndrome
Cushing’s Syndrome refers to a clinical state of prolonged glucocorticoid excess, regardless of cause. It may result from exogenous steroid use or endogenous overproduction of cortisol. When specifically caused by an ACTH-secreting pituitary adenoma, it is referred to as Cushing’s Disease. This condition is associated with significant metabolic, cardiovascular, and musculoskeletal complications and must be recognised early to prevent morbidity.
Definition
- Cushing’s Syndrome: A collection of signs and symptoms resulting from chronic exposure to excess glucocorticoids.
- Cushing’s Disease: A subtype of Cushing’s Syndrome caused by an ACTH-producing pituitary adenoma (central cause).
Aetiology
- Exogenous (most common):
- Prolonged corticosteroid therapy
- Endogenous causes:
- Cushing’s Disease – ACTH-secreting pituitary adenoma
- Ectopic ACTH production (e.g. small cell lung carcinoma)
- Adrenal adenoma or carcinoma (ACTH-independent)
Pathophysiology (Cushing’s Disease)
- ACTH-secreting pituitary adenoma → ↑ACTH → Stimulates adrenal cortex → ↑Cortisol
- Cortisol excess exerts widespread effects on metabolism, blood pressure, immune function, and connective tissue.
Clinical Features
- Onset: Gradual
- Early signs:
- Weight gain (especially central/truncal obesity)
- Hypertension
- Classic features:
- “Moon face” (facial rounding)
- “Buffalo hump” (posterior cervical fat pad)
- Abdominal striae (purple stretch marks)
- Proximal muscle weakness
- Thin skin & easy bruising
- Hirsutism (in females)
- Acne
- Osteopenia/osteoporosis
- Menstrual irregularities
- Depression or psychosis
- Insulin resistance → hyperglycaemia or type 2 diabetes
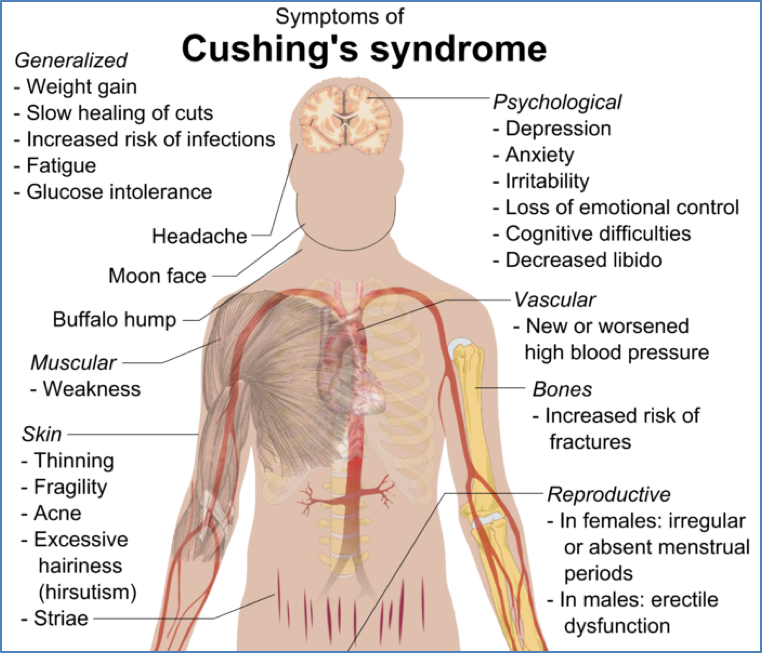

Ozlem Celik, Mutlu Niyazoglu, Hikmet Soylu and Pinar Kadioglu, CC BY 2.5 <https://creativecommons.org/licenses/by/2.5>, via Wikimedia Commons
Investigations
- Initial screening:
- 24hr urinary free cortisol
- Midnight salivary cortisol
- Low-dose dexamethasone suppression test
- To determine cause:
- Serum ACTH levels:
- ↑ACTH → ACTH-dependent (pituitary or ectopic source)
- ↓ACTH → ACTH-independent (adrenal cause)
- High-dose dexamethasone suppression test:
- Suppression → Suggests pituitary (Cushing’s Disease)
- No suppression → Suggests ectopic ACTH production
- MRI brain → Pituitary tumour
- CT adrenal glands → For suspected adrenal tumours
- Serum ACTH levels:
Management
- Exogenous Cushing’s Syndrome:
- Gradual tapering of corticosteroids
- Cushing’s Disease (Pituitary Adenoma):
- Trans-sphenoidal surgical resection
- Temporary cortisol replacement post-op
- Consider radiation or medical therapy if surgery fails
- Adrenal adenoma/carcinoma:
- Surgical removal + cortisol replacement
- Ectopic ACTH production:
- Identify and treat underlying tumour
Complications
- Type 2 diabetes mellitus
- Hypertension
- Osteoporosis
- Cardiovascular disease
- Opportunistic infections
- Adrenal insufficiency post-treatment
Summary – Cushing’s Syndrome
Cushing’s Syndrome is a condition of chronic glucocorticoid excess with systemic complications, most often iatrogenic in origin. Cushing’s Disease, caused by a pituitary adenoma, is a notable endogenous subtype. Diagnosis hinges on cortisol/ACTH levels and suppression testing, while management involves addressing the underlying source of hormone excess. For related conditions, visit our Endocrine Overview.